
- Test for Panic Disorder
- Online Therapy for Panic and Anxiety
- Test for Social Anxiety Disorder
- Online Therapy for Social Anxiety
- Generalized Anxiety
- Post-Traumatic Stress Disorder
- Selective Mutism
- Obsessive-Compulsive Disorder
- Help & Support
- Test for Social Anxiety

You are here
- Social Phobia/Anxiety Case Study: Jim
Jim was a nice looking man in his mid-30’s. He could trace his shyness to boyhood and his social anxiety to his teenage years. He had married a girl he knew well from high school and had almost no other dating history. He and his wife, Lesley, had three children, two girls and a boy.
At our first meeting, Jim was very shy and averted his eyes from me, but he did shake hands, respond, and smile a genuine smile. A few minutes into our session and Jim was noticeably more relaxed. "I’ve suffered with this anxiety for as long as I can remember", he said. "Even in school, I was backward and didn’t know what to say. After I got married, my wife started taking over all of the daily, family responsibilities and I was more than glad to let her."
If there was an appointment to be made, Lesley made it. If there was a parent-teacher conference to go to, Lesley went to it. If Jim had something coming up, Lesley would make all the social arrangements. Even when the family ordered takeout food, it was Lesley who made the call. Jim was simply too afraid and shy.
Indeed, because of his wife, Jim was able to avoid almost all social responsibility -- except at his job. It was his job and its responsibilities that brought Jim into treatment.
Years earlier, Jim had worked at a small, locally-owned record and tape store, where he knew the owner and felt a part of the family. The business was slow and manageable and he never found himself on display in front of lines of people. Several years previously, however, the owner had sold his business to a national record chain, and Jim found himself a lower mid-range manager in a national corporation, a position he did not enjoy.
"When I have to call people up to tell them that their order is in," he said, "I know my voice is going to be weak and break, and I will be unable to get my words out. I’ll stumble around and choke up....then I’ll blurt out the rest of my message so fast I’m afraid they won’t understand me. Sometimes I have to repeat myself and that is excruciatingly embarrassing........"
Jim felt great humiliation and embarrassment about this afterwards: he couldn’t even make a telephone call to a stranger without getting extremely anxious and giving himself away. That was pretty bad! Then he would beat himself up. What was wrong with him? Why was he so timid and scared? No one else seemed to be like he was. He simply must be crazy! After a day full of this pressure, anxiety and negative thinking, Jim would leave work feeling fatigued, tired, and defeated.
Meanwhile, his wife, being naturally sociable and vocal, continually enabled Jim not to have to deal with any social situations. In restaurants, his wife always ordered. At home, she answered the telephone and made all the calls out. He would tell her things that needed to be done and she would do them.
He had no friends of his own, except for the couples his wife knew from her work. At times when he felt he simply had to go to these social events, Jim was very ill-at-ease, never knew what to say, and felt the silences that occurred in conversation were his fault for being so backward. He knew he made everyone else uncomfortable and ill-at-ease.
Of course, the worst part of all was the anticipatory anxiety Jim felt ahead of time – when he knew he had to perform, do something in public, or even make phone calls from work. The more time he had to worry and stew about these situations, the more anxious, fearful and uncomfortable he felt.
REMARKS: Jim presented a very typical case of generalized social phobia/social anxiety. His strong anticipation and belief that he wouldn’t do well at social interactions and in social events became a self-fulfilling prophecy, and his belief came true: he didn’t do well. The more nervous and anxious he got over a situation, and the more attention he paid to it, the more he could not perform well. This was a very negative paradox or "vicious cycle" that all people with social anxiety get stuck in. If your beliefs are strong that you will NOT do well, then it is likely you will not do well. Therefore, thoughts, beliefs, and emotions need to be changed.
The depression (technically "dysthymia") that comes about after the anxious event continued to fuel the fire. "I’ll never be able to deal with this," Jim would tell himself, thus constantly reinforcing the fact that he saw himself as a failure and a loser.
Unusual in this situation is that Jim’s wife remained loyal to him, understood his problem to some extent, and even seemed to enjoy her role as the family’s "social director". The more and more she did for Jim, the more and more he could avoid. It got so bad that Jim, who loved to listen to new albums and read new books -- could not even go to stores or to the library. He would tell his wife what to buy and she would buy it. She even kept track of when the library books were due and made sure she took them back on time.
This family situation is unusual because most people with social anxiety/social phobia have an extremely difficult time making and continuing personal relationships -- because of self-consciousness and the need for more privacy than most other people. In fact, social phobia ranks among one of the highest psychological disorders when it comes to failed relationships, divorce, and living alone.
TREATMENT for Jim consisted of the normal course of cognitive strategies so that he would relearn and rethink what he was doing to himself. He was cooperative from the beginning, and progressed nicely doing therapy. He took each of the practice handouts and spent time each day practicing. He made a "special time" for himself that his family respected and he used this place and time to practice the cognitive strategies his mind had to learn.
His biggest real-life fear, speaking to another person in public, was not really a speaking problem; it was an anxiety problem. There was nothing wrong with Jim’s voice, his reading ability, or his speaking ability. Jim was a bright man who had associated great anxiety around these social events in public situations.
The course of treatment here is NOT to practice! In fact, practicing would just draw attention to what Jim perceived was the problem: his voice, his awkwardness, his perceived inability to speak to others. Thus, it would reinforce the very behaviors we do not want to reinforce.
Instead, Jim worked on paradoxes. We deliberately goofed-up. We tried to make as many mistakes as possible. We injected humor into the situation and found that when he exaggerated his fears, he thought this was funny. Although more is involved than just this, the concept here is to de-stress the situation and enable the person to see it for what it is: NO BIG DEAL! If you make a mistake, SO WHAT? Everyone else does too!
Over the weeks, before group therapy began, Jim did a number of interesting things in public that began proving to him that he was NOT the center of attention, and it just didn’t matter if he made a mistake or two. After all, he was human just like everyone else. It’s this idea of perfectionism, of always having to "do your best" that must be broken down. Jim was human; humans make mistakes; so what? It was certainly nothing to get upset about. In fact, as time went by, it become even more funny and humorous, rather than humiliating or embarrassing.
After completion of the behavioral group therapy, Jim had an opportunity for advancement in his company, which he now felt comfortable to take. The promotion entailed holding weekly meetings in which he was in charge. He would have to do some public speaking and respond to his employees’ questions. By this time, Jim was feeling much more comfortable and much less anxious about the whole situation. "I think I’ll deliberately goof up," he joked to me before the start of his new job. "It would be interesting to see how everyone else responds."
To say that Jim did not have any anticipatory anxiety before taking this position or before making his weekly presentations would be inaccurate. The difference was now they were manageable. They were simply minor roadblocks that could be overcome. Jim’s thinking about social events and activities had changed a great deal since the first day I saw him in therapy.
I talked to Jim a few months ago and everything was going well. His responsibilities at work had increased slightly, but Jim now had the ability and beliefs to deal with them. He was much more confident and had a feeling of being in control. He was doing more around the house and his wife was a little surprised at his metamorphosis. Luckily, this did not change the marriage dynamics adversely, and the last time I talked with him, Jim had become a father again: another little boy.
"He’s the last," Jim said, laughing over the phone, "I can’t get too distracted. I’ve got too many speeches to give now."
- social anxiety
- anxiety disorder

Social Anxiety
- A New Test for Social Anxiety Disorder
- Why We Prefer "Social Anxiety" to "Social Phobia"
- Visiting The Social Anxiety Therapy Group
- Thinking Problems: Correcting Our Misperceptions
- What is Social Anxiety/Social Phobia?
- Personal Statements for Social Anxiety
- The Scorpion's Sting: An Anxiety Parable
- Social Anxiety Questions and Answers
- Social Anxiety and Misdiagnosis
- Social Anxiety Disorder and Medication
- The Least Understood Anxiety Disorder
- What are "The Phobias"?
- Social Anxiety: Past and Present
- What is the Difference Between Panic Disorder and Social Anxiety Disorder?
- Ask Dr. Richards About Anxiety Disorders
Latest articles

- Depression and Anxiety Survey

Our History and Our Mission
The Anxiety Network began in 1995 due to growing demand from people around the world wanting help in understanding and overcoming their anxiety disorder. The Anxiety Clinic of Arizona and its website, The Anxiety Network, received so much traffic and requests for help that we found ourselves spending much of our time in international communication and outreach. Our in-person anxiety clinic has grown tremendously, and our principal internet tool, The Anxiety Network, has been re-written and re-designed with focus on the three major anxiety disorders: panic, social anxiety, and generalized anxiety disorder.
The Anxiety Network focuses on three of the major anxiety disorders: panic disorder, generalized anxiety disorder, and social anxiety disorder.
In 1997, The Social Anxiety Association , a non-profit organization, was formed and now has its own website.
The Social Anxiety Institute , the largest site on the internet for information and treatment of social anxiety, has maintained an active website since 1998. Continuous, ongoing therapy groups have helped hundreds of people overcome social anxiety since 1994.
Site Navigation
- Anxiety Help and Support
- Bookstore and Digital Downloads
- Panic Disorder, with and without Agoraphobia
- Generalized Anxiety Disorder Information
- Social Anxiety Disorder Information
- Post-Traumatic-Stress-Disorder
Follow Dr. Richards
© 1995, 2020, The Anxiety Network
Thomas A. Richards, Ph.D., Psychologist/Founder
Matthew S. Whitley, M.B.A., Program Coordinator/Therapist

Social Anxiety Disorder: A Comprehensive Case Study Analysis
Hearts racing and minds reeling, millions navigate a world where everyday interactions feel like walking through a minefield of judgment and scrutiny. This pervasive experience is the hallmark of social anxiety disorder, a condition that affects countless individuals worldwide, impacting their daily lives and overall well-being. To truly understand the complexities of this disorder and develop effective treatment strategies, researchers and clinicians often turn to case studies, which provide invaluable insights into the lived experiences of those grappling with social anxiety.
Understanding Social Anxiety Disorder
Social anxiety disorder, also known as social phobia, is characterized by an intense and persistent fear of social situations. Individuals with this condition experience overwhelming anxiety and self-consciousness in everyday social interactions, often fearing negative judgment or embarrassment. The impact of social anxiety extends far beyond mere shyness, significantly interfering with personal relationships, professional opportunities, and overall quality of life.
The prevalence of social anxiety disorder is staggering, affecting an estimated 7% of the global population. This translates to millions of individuals worldwide who struggle with the debilitating effects of this condition. From avoiding social gatherings to experiencing panic attacks in public spaces, the manifestations of social anxiety can be both diverse and profound.
To truly grasp the nuances of social anxiety disorder and develop effective treatment approaches, clinicians and researchers rely heavily on case studies. These in-depth analyses of individual experiences provide a wealth of information that cannot be captured by statistical data alone. By examining specific cases, professionals can identify patterns, explore unique manifestations, and refine treatment strategies to better serve those affected by social anxiety.
Case Study Background: Meet Sarah
In this comprehensive case study analysis, we’ll delve into the experience of Sarah, a 28-year-old marketing professional who has been grappling with social anxiety disorder for over a decade. Sarah’s journey offers valuable insights into the onset, progression, and treatment of this challenging condition.
Sarah grew up in a small town in the Midwest, describing herself as a shy and introverted child. While she had a close-knit group of friends throughout her school years, she often felt uncomfortable in large social gatherings or when required to speak in front of her class. However, it wasn’t until her college years that her anxiety began to escalate significantly.
The onset of Sarah’s more severe social anxiety symptoms coincided with her move to a large university in a bustling city. Suddenly thrust into an environment where she knew no one, Sarah found herself overwhelmed by the constant social interactions required in her new setting. She began experiencing intense physical symptoms, including rapid heartbeat, sweating, and trembling, whenever she had to participate in class discussions or attend social events.
As her symptoms worsened, Sarah sought help from the university’s counseling center. After a thorough assessment process, including interviews, questionnaires, and comprehensive social anxiety disorder tests , Sarah was diagnosed with social anxiety disorder. This diagnosis marked the beginning of her journey towards understanding and managing her condition.
Symptoms and Manifestations
Sarah’s experience with social anxiety disorder manifested in a variety of physical, cognitive, and behavioral symptoms. Physically, she reported experiencing:
1. Rapid heartbeat and palpitations 2. Excessive sweating, particularly on her palms and forehead 3. Trembling or shaking, especially in her hands 4. Nausea and stomach discomfort 5. Difficulty breathing or a sensation of choking
These physical symptoms often intensified in situations where Sarah felt she was being observed or evaluated, such as during presentations at work or when meeting new people.
Cognitively, Sarah’s social anxiety was characterized by persistent negative thought patterns and beliefs. She frequently experienced:
1. Intense fear of judgment or criticism from others 2. Excessive self-consciousness and hyper-awareness of her actions 3. Negative self-talk and self-criticism 4. Catastrophic thinking about potential social failures 5. Difficulty concentrating in social situations due to racing thoughts
These cognitive patterns significantly impacted Sarah’s ability to engage in social interactions and professional activities, often leading to a cycle of avoidance and increased anxiety.
Behaviorally, Sarah developed various avoidance strategies to cope with her anxiety. These included:
1. Declining invitations to social events or gatherings 2. Avoiding eye contact or speaking up in meetings at work 3. Using alcohol as a social lubricant to ease her anxiety 4. Overpreparation for presentations or social interactions to minimize potential mistakes 5. Relying heavily on digital communication to avoid face-to-face interactions
While these avoidance strategies provided temporary relief, they ultimately reinforced Sarah’s anxiety and limited her personal and professional growth.
Treatment Approach
Upon receiving her diagnosis, Sarah began a comprehensive treatment plan that incorporated both psychotherapy and medication management. The primary therapeutic approach used was Cognitive-Behavioral Therapy (CBT), a well-established and effective treatment for social anxiety disorder.
CBT sessions focused on helping Sarah identify and challenge her negative thought patterns and beliefs about social situations. Her therapist employed various techniques, including:
1. Cognitive restructuring to help Sarah recognize and reframe irrational thoughts 2. Mindfulness exercises to increase awareness of her anxiety symptoms and reduce their intensity 3. Role-playing exercises to practice social skills and build confidence 4. Gradual exposure to anxiety-provoking situations in a controlled environment
In addition to CBT, Sarah’s treatment plan included group therapy sessions specifically designed for individuals with social anxiety . These sessions provided a supportive environment where Sarah could practice social interactions and learn from others facing similar challenges.
To address the physical symptoms of her anxiety, Sarah’s psychiatrist prescribed a selective serotonin reuptake inhibitor (SSRI), which helped reduce the intensity of her anxiety symptoms and improved her overall mood.
A crucial component of Sarah’s treatment was exposure therapy, which involved gradually facing feared social situations in a structured and supported manner. This approach helped Sarah build confidence and develop more adaptive coping strategies. Some exposure exercises included:
1. Initiating conversations with strangers in low-pressure settings 2. Participating in social events without using alcohol as a crutch 3. Volunteering to lead presentations at work 4. Attending networking events in her industry
Throughout her treatment, Sarah also engaged in social skills training to improve her ability to navigate various social situations with greater ease and confidence.
Progress and Outcomes
As Sarah progressed through her treatment, she began to experience significant improvements in her social functioning and overall quality of life. In the short term, she reported:
1. Reduced physical symptoms of anxiety in social situations 2. Increased willingness to engage in social activities 3. Improved performance and confidence at work 4. Better ability to challenge and reframe negative thoughts
Over the long term, Sarah developed more effective strategies for managing her symptoms and maintaining her progress. She continued to practice the skills learned in therapy and gradually expanded her social circle. While she still experienced occasional anxiety in certain situations, she felt better equipped to handle these challenges without resorting to avoidance behaviors.
From Sarah’s perspective, the combination of CBT, medication, and exposure therapy was instrumental in her recovery. She particularly valued the practical skills she gained through therapy, which allowed her to approach social situations with greater confidence and self-compassion.
Analysis and Insights
Sarah’s case study offers valuable insights into the treatment of social anxiety disorder and highlights several key factors contributing to her success:
1. Comprehensive approach: The combination of psychotherapy, medication, and exposure techniques addressed multiple aspects of Sarah’s anxiety.
2. Personalized treatment plan: Sarah’s therapy was tailored to her specific needs and experiences, focusing on the situations that caused her the most distress.
3. Gradual exposure: The step-by-step approach to facing feared situations allowed Sarah to build confidence incrementally.
4. Skill development: Learning practical social skills and cognitive techniques provided Sarah with tools to manage her anxiety in real-world situations.
5. Supportive environment: Group therapy sessions offered a safe space for Sarah to practice social interactions and gain support from peers.
Despite the overall success of Sarah’s treatment, there were challenges encountered along the way. These included:
1. Initial resistance to exposure exercises due to fear of discomfort 2. Difficulty in consistently applying cognitive techniques during high-stress situations 3. Occasional setbacks or temporary increases in anxiety symptoms
Addressing these challenges required patience, persistence, and ongoing support from Sarah’s treatment team.
The insights gained from Sarah’s case have important implications for future social anxiety disorder case studies and treatment approaches. They highlight the need for:
1. Individualized treatment plans that address the unique manifestations of social anxiety in each patient 2. A focus on long-term skill development and coping strategies, rather than just symptom reduction 3. Integration of various therapeutic modalities to address different aspects of the disorder 4. Ongoing support and follow-up to maintain progress and prevent relapse
Sarah’s journey with social anxiety disorder illustrates the complex nature of this condition and the potential for significant improvement with appropriate treatment. Her case underscores the importance of a comprehensive, individualized approach that combines evidence-based therapies, medication when necessary, and ongoing support.
As research in the field of social anxiety continues to evolve, case studies like Sarah’s provide invaluable insights that inform future treatment strategies. They remind us that while social anxiety disorder can be a challenging condition, it is also highly treatable. With the right support and interventions, individuals like Sarah can learn to manage their symptoms effectively and lead fulfilling lives.
Looking ahead, the field of social anxiety research and treatment continues to advance. Emerging areas of focus include:
1. The role of virtual reality in exposure therapy for social anxiety 2. The potential of mindfulness-based interventions in managing anxiety symptoms 3. Exploration of the relationship between social anxiety and related conditions like OCD 4. Investigation into the potential benefits of social anxiety in certain contexts
As our understanding of social anxiety disorder deepens, so too does our ability to provide effective, compassionate care to those affected by this condition. Sarah’s story serves as a testament to the power of perseverance, evidence-based treatment, and the human capacity for growth and change in the face of significant challenges.
For individuals struggling with social anxiety, it’s important to remember that help is available. Whether you’re experiencing high-functioning social anxiety or more severe symptoms, seeking professional support can be a crucial first step towards managing your condition and improving your quality of life. With the right tools and support, it’s possible to navigate the complexities of social anxiety and build a life filled with meaningful connections and personal growth.
References:
1. American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing.
2. Heimberg, R. G., Brozovich, F. A., & Rapee, R. M. (2010). A cognitive behavioral model of social anxiety disorder: Update and extension. In S. G. Hofmann & P. M. DiBartolo (Eds.), Social anxiety: Clinical, developmental, and social perspectives (2nd ed., pp. 395-422). Academic Press.
3. National Institute of Mental Health. (2022). Social Anxiety Disorder: More Than Just Shyness. https://www.nimh.nih.gov/health/publications/social-anxiety-disorder-more-than-just-shyness
4. Stein, M. B., & Stein, D. J. (2008). Social anxiety disorder. The Lancet, 371(9618), 1115-1125.
5. Clark, D. M., & Wells, A. (1995). A cognitive model of social phobia. In R. G. Heimberg, M. R. Liebowitz, D. A. Hope, & F. R. Schneier (Eds.), Social phobia: Diagnosis, assessment, and treatment (pp. 69-93). The Guilford Press.
6. Hofmann, S. G., & Otto, M. W. (2017). Cognitive behavioral therapy for social anxiety disorder: Evidence-based and disorder-specific treatment techniques. Routledge.
7. Craske, M. G., Niles, A. N., Burklund, L. J., Wolitzky-Taylor, K. B., Vilardaga, J. C., Arch, J. J., … & Lieberman, M. D. (2014). Randomized controlled trial of cognitive behavioral therapy and acceptance and commitment therapy for social phobia: Outcomes and moderators. Journal of Consulting and Clinical Psychology, 82(6), 1034-1048.
8. Goldin, P. R., Morrison, A., Jazaieri, H., Brozovich, F., Heimberg, R., & Gross, J. J. (2016). Group CBT versus MBSR for social anxiety disorder: A randomized controlled trial. Journal of Consulting and Clinical Psychology, 84(5), 427-437.
9. Kessler, R. C., Petukhova, M., Sampson, N. A., Zaslavsky, A. M., & Wittchen, H. U. (2012). Twelve‐month and lifetime prevalence and lifetime morbid risk of anxiety and mood disorders in the United States. International Journal of Methods in Psychiatric Research, 21(3), 169-184.
10. Ruscio, A. M., Brown, T. A., Chiu, W. T., Sareen, J., Stein, M. B., & Kessler, R. C. (2008). Social fears and social phobia in the USA: results from the National Comorbidity Survey Replication. Psychological Medicine, 38(1), 15-28.
Similar Posts

Mastering Anxiety: Powerful Coping Statements to Reclaim Your Peace of Mind
Silencing the cacophony of worry, a simple yet potent tool awaits those ready to reclaim their mental tranquility. Anxiety, a pervasive and often debilitating condition, affects millions of people worldwide, impacting their daily lives, relationships, and overall well-being. However, amidst the turmoil of anxious thoughts, there exists a powerful technique that can help individuals regain…

Overcoming the Phobia of Smelling Bad: Understanding and Managing Olfactory Anxiety
Nose twitching and palms sweating, Sarah scrutinized every passerby’s face for signs of disgust, convinced her imaginary stench was repelling the entire subway car. This scene, all too familiar for those suffering from olfactory anxiety, illustrates the debilitating nature of the fear of smelling bad. This phobia, often overlooked or dismissed as mere vanity, can…

Understanding and Helping Dogs with Social Anxiety: A Comprehensive Guide
Trembling paws and tucked tails tell a tale of canine torment that millions of pet owners struggle to decipher and resolve. Social anxiety in dogs is a complex and often misunderstood condition that can significantly impact the lives of both pets and their owners. This pervasive issue affects countless canines worldwide, manifesting in various ways…

50 Powerful Social Anxiety Journal Prompts to Boost Your Confidence and Overcome Fear
Pen poised over paper, you tremble at the thought of social interaction—but these 50 powerful journal prompts are about to transform your fear into unshakeable confidence. Social anxiety can be a debilitating condition that affects millions of people worldwide, making everyday interactions feel like insurmountable challenges. However, there’s a powerful tool at your disposal that…

The Complex Relationship Between Social Anxiety and Perfectionism: Understanding and Overcoming the Dual Challenge
Perfectionism’s relentless pursuit of flawlessness and social anxiety’s paralyzing fear of judgment dance a torturous tango in the minds of millions, each step amplifying the other’s intensity. This intricate interplay between two seemingly distinct psychological phenomena creates a complex web of thoughts, emotions, and behaviors that can significantly impact an individual’s quality of life. To…

The Anxiety Podcast: A Comprehensive Guide to Understanding and Managing Anxiety
Tune in to tranquility as the airwaves become an unexpected sanctuary for millions grappling with the relentless grip of anxiety. In recent years, the world of podcasting has emerged as a powerful tool for those seeking solace, understanding, and practical strategies to manage their anxiety. As the prevalence of anxiety disorders continues to rise globally,…
Leave a Reply Cancel reply
Your email address will not be published. Required fields are marked *
Save my name, email, and website in this browser for the next time I comment.
- Patient Care & Health Information
- Diseases & Conditions
- Social anxiety disorder (social phobia)
It's normal to feel nervous in some social situations. For example, going on a date or giving a presentation may cause that feeling of butterflies in your stomach. But in social anxiety disorder, also called social phobia, everyday interactions cause significant anxiety, self-consciousness and embarrassment because you fear being scrutinized or judged negatively by others.
In social anxiety disorder, fear and anxiety lead to avoidance that can disrupt your life. Severe stress can affect your relationships, daily routines, work, school or other activities.
Social anxiety disorder can be a chronic mental health condition, but learning coping skills in psychotherapy and taking medications can help you gain confidence and improve your ability to interact with others.
Social anxiety disorder care at Mayo Clinic
Products & Services
- A Book: Mayo Clinic Family Health Book
- Newsletter: Mayo Clinic Health Letter — Digital Edition
Feelings of shyness or discomfort in certain situations aren't necessarily signs of social anxiety disorder, particularly in children. Comfort levels in social situations vary, depending on personality traits and life experiences. Some people are naturally reserved and others are more outgoing.
In contrast to everyday nervousness, social anxiety disorder includes fear, anxiety and avoidance that interfere with relationships, daily routines, work, school or other activities. Social anxiety disorder typically begins in the early to mid-teens, though it can sometimes start in younger children or in adults.
Emotional and behavioral symptoms
Signs and symptoms of social anxiety disorder can include constant:
- Fear of situations in which you may be judged negatively
- Worry about embarrassing or humiliating yourself
- Intense fear of interacting or talking with strangers
- Fear that others will notice that you look anxious
- Fear of physical symptoms that may cause you embarrassment, such as blushing, sweating, trembling or having a shaky voice
- Avoidance of doing things or speaking to people out of fear of embarrassment
- Avoidance of situations where you might be the center of attention
- Anxiety in anticipation of a feared activity or event
- Intense fear or anxiety during social situations
- Analysis of your performance and identification of flaws in your interactions after a social situation
- Expectation of the worst possible consequences from a negative experience during a social situation
For children, anxiety about interacting with adults or peers may be shown by crying, having temper tantrums, clinging to parents or refusing to speak in social situations.
Performance type of social anxiety disorder is when you experience intense fear and anxiety during speaking or performing in public but not in other types of more general social situations.
Physical symptoms
Physical signs and symptoms can sometimes accompany social anxiety disorder and may include:
- Fast heartbeat
- Upset stomach or nausea
- Trouble catching your breath
- Dizziness or lightheadedness
- Feeling that your mind has gone blank
- Muscle tension
Avoiding common social situations
Common, everyday experiences may be hard to endure when you have social anxiety disorder, including:
- Interacting with unfamiliar people or strangers
- Attending parties or social gatherings
- Going to work or school
- Starting conversations
- Making eye contact
- Entering a room in which people are already seated
- Returning items to a store
- Eating in front of others
- Using a public restroom
Social anxiety disorder symptoms can change over time. They may flare up if you're facing a lot of changes, stress or demands in your life. Although avoiding situations that produce anxiety may make you feel better in the short term, your anxiety is likely to continue over the long term if you don't get treatment.
When to see a doctor
See your doctor or a mental health professional if you fear and avoid normal social situations because they cause embarrassment, worry or panic.
There is a problem with information submitted for this request. Review/update the information highlighted below and resubmit the form.
From Mayo Clinic to your inbox
Sign up for free and stay up to date on research advancements, health tips, current health topics, and expertise on managing health. Click here for an email preview.
Error Email field is required
Error Include a valid email address
To provide you with the most relevant and helpful information, and understand which information is beneficial, we may combine your email and website usage information with other information we have about you. If you are a Mayo Clinic patient, this could include protected health information. If we combine this information with your protected health information, we will treat all of that information as protected health information and will only use or disclose that information as set forth in our notice of privacy practices. You may opt-out of email communications at any time by clicking on the unsubscribe link in the e-mail.
Thank you for subscribing!
You'll soon start receiving the latest Mayo Clinic health information you requested in your inbox.
Sorry something went wrong with your subscription
Please, try again in a couple of minutes
Like many other mental health conditions, social anxiety disorder likely arises from a complex interaction of biological and environmental factors. Possible causes include:
- Inherited traits. Anxiety disorders tend to run in families. However, it isn't entirely clear how much of this may be due to genetics and how much is due to learned behavior.
- Brain structure. A structure in the brain called the amygdala (uh-MIG-duh-luh) may play a role in controlling the fear response. People who have an overactive amygdala may have a heightened fear response, causing increased anxiety in social situations.
- Environment. Social anxiety disorder may be a learned behavior — some people may develop significant anxiety after an unpleasant or embarrassing social situation. Also, there may be an association between social anxiety disorder and parents who either model anxious behavior in social situations or are more controlling or overprotective of their children.
Risk factors
Several factors can increase the risk of developing social anxiety disorder, including:
- Family history. You're more likely to develop social anxiety disorder if your biological parents or siblings have the condition.
- Negative experiences. Children who experience teasing, bullying, rejection, ridicule or humiliation may be more prone to social anxiety disorder. In addition, other negative events in life, such as family conflict, trauma or abuse, may be associated with this disorder.
- Temperament. Children who are shy, timid, withdrawn or restrained when facing new situations or people may be at greater risk.
- New social or work demands. Social anxiety disorder symptoms typically start in the teenage years, but meeting new people, giving a speech in public or making an important work presentation may trigger symptoms for the first time.
- Having an appearance or condition that draws attention. For example, facial disfigurement, stuttering or tremors due to Parkinson's disease can increase feelings of self-consciousness and may trigger social anxiety disorder in some people.
Complications
Left untreated, social anxiety disorder can control your life. Anxieties can interfere with work, school, relationships or enjoyment of life. This disorder can cause:
- Low self-esteem
- Trouble being assertive
- Negative self-talk
- Hypersensitivity to criticism
- Poor social skills
- Isolation and difficult social relationships
- Low academic and employment achievement
- Substance abuse, such as drinking too much alcohol
- Suicide or suicide attempts
Other anxiety disorders and certain other mental health disorders, particularly major depressive disorder and substance abuse problems, often occur with social anxiety disorder.
There's no way to predict what will cause someone to develop an anxiety disorder, but you can take steps to reduce the impact of symptoms if you're anxious:
- Get help early. Anxiety, like many other mental health conditions, can be harder to treat if you wait.
- Keep a journal. Keeping track of your personal life can help you and your mental health professional identify what's causing you stress and what seems to help you feel better.
- Set priorities in your life. You can reduce anxiety by carefully managing your time and energy. Make sure that you spend time doing things you enjoy.
- Avoid unhealthy substance use. Alcohol and drug use and even caffeine or nicotine use can cause or worsen anxiety. If you're addicted to any of these substances, quitting can make you anxious. If you can't quit on your own, see your health care provider or find a treatment program or support group to help you.
Social anxiety disorder (social phobia) care at Mayo Clinic
- Social anxiety disorder (social phobia). In: Diagnostic and Statistical Manual of Mental Disorders DSM-5. 5th ed. American Psychiatric Association; 2013. http://dsm.psychiatryonline.org. Accessed May 21, 2021.
- Gabbard GO, ed. Social anxiety disorder (social phobia). In: Gabbard's Treatments of Psychiatric Disorders. 5th ed. American Psychiatric Association; 2014. http://psychiatryonline.org/doi/book/10.1176/appi.books.9781585625048. Accessed May 21, 2021.
- Schneier FR. Social anxiety disorder in adults: Epidemiology, clinical manifestations, and diagnosis. https://www.uptodate.com/contents/search. Accessed April 8, 2021.
- Stein MB, et al. Approach to treating social anxiety disorder in adults. https://www.uptodate.com/contents/search. Accessed April 8, 2021.
- Hofmann SG. Psychotherapy for social anxiety disorder in adults. https://www.uptodate.com/contents/search. Accessed April 8, 2021.
- Stein MB. Pharmacotherapy for social anxiety disorder in adults. https://www.uptodate.com/contents/search. Accessed April 8, 2021.
- Bystritsky A. Complementary and alternative treatments for anxiety symptoms and disorders: Herbs and medications. https://www.uptodate.com/contents/search. Accessed April 8, 2021.
- Bystritsky A. Complementary and alternative treatments for anxiety symptoms and disorders: Physical, cognitive, and spiritual interventions. https://www.uptodate.com/contents/search. Accessed April 8, 2021.
- Social anxiety disorder: More than just shyness. National Institute of Mental Health. https://www.nimh.nih.gov/health/publications/social-anxiety-disorder-more-than-just-shyness/index.shtml. Accessed April 8, 2021.
- Natural medicines in the clinical management of anxiety. Natural Medicines. https://naturalmedicines.therapeuticresearch.com. Accessed April 8, 2021.
- Sawchuk CN (expert opinion). Mayo Clinic. April 29, 2021.
- AskMayoExpert. Anxiety disorders. Mayo Clinic; 2020. Accessed April 8, 2021.
- Brown A. Allscripts EPSi. Mayo Clinic. Sept. 11, 2020.
- Valerian. Natural Medicines. https://naturalmedicines.therapeuticresearch.com. Accessed April 12, 2021.
- Sarris J, et al., eds. Anxiety. In: Clinical Naturopathy. 3rd ed. Elsevier; 2019. https://www.clinicalkey.com. Accessed April 12, 2021.
Associated Procedures
- Cognitive behavioral therapy
- Psychotherapy
- Symptoms & causes
- Diagnosis & treatment
- Doctors & departments
- Care at Mayo Clinic
Mayo Clinic does not endorse companies or products. Advertising revenue supports our not-for-profit mission.
- Opportunities
Mayo Clinic Press
Check out these best-sellers and special offers on books and newsletters from Mayo Clinic Press .
- Mayo Clinic on Incontinence - Mayo Clinic Press Mayo Clinic on Incontinence
- The Essential Diabetes Book - Mayo Clinic Press The Essential Diabetes Book
- Mayo Clinic on Hearing and Balance - Mayo Clinic Press Mayo Clinic on Hearing and Balance
- FREE Mayo Clinic Diet Assessment - Mayo Clinic Press FREE Mayo Clinic Diet Assessment
- Mayo Clinic Health Letter - FREE book - Mayo Clinic Press Mayo Clinic Health Letter - FREE book
5X Challenge
Thanks to generous benefactors, your gift today can have 5X the impact to advance AI innovation at Mayo Clinic.
- Search Menu
Sign in through your institution
- Browse content in Arts and Humanities
- Browse content in Archaeology
- Anglo-Saxon and Medieval Archaeology
- Archaeological Methodology and Techniques
- Archaeology by Region
- Archaeology of Religion
- Archaeology of Trade and Exchange
- Biblical Archaeology
- Contemporary and Public Archaeology
- Environmental Archaeology
- Historical Archaeology
- History and Theory of Archaeology
- Industrial Archaeology
- Landscape Archaeology
- Mortuary Archaeology
- Prehistoric Archaeology
- Underwater Archaeology
- Zooarchaeology
- Browse content in Architecture
- Architectural Structure and Design
- History of Architecture
- Residential and Domestic Buildings
- Theory of Architecture
- Browse content in Art
- Art Subjects and Themes
- History of Art
- Industrial and Commercial Art
- Theory of Art
- Biographical Studies
- Byzantine Studies
- Browse content in Classical Studies
- Classical Philosophy
- Classical Mythology
- Classical History
- Classical Reception
- Classical Numismatics
- Classical Literature
- Classical Art and Architecture
- Classical Oratory and Rhetoric
- Greek and Roman Epigraphy
- Greek and Roman Law
- Greek and Roman Papyrology
- Greek and Roman Archaeology
- Late Antiquity
- Religion in the Ancient World
- Social History
- Digital Humanities
- Browse content in History
- Colonialism and Imperialism
- Diplomatic History
- Environmental History
- Genealogy, Heraldry, Names, and Honours
- Genocide and Ethnic Cleansing
- Historical Geography
- History by Period
- History of Emotions
- History of Agriculture
- History of Education
- History of Gender and Sexuality
- Industrial History
- Intellectual History
- International History
- Labour History
- Legal and Constitutional History
- Local and Family History
- Maritime History
- Military History
- National Liberation and Post-Colonialism
- Oral History
- Political History
- Public History
- Regional and National History
- Revolutions and Rebellions
- Slavery and Abolition of Slavery
- Social and Cultural History
- Theory, Methods, and Historiography
- Urban History
- World History
- Browse content in Language Teaching and Learning
- Language Learning (Specific Skills)
- Language Teaching Theory and Methods
- Browse content in Linguistics
- Applied Linguistics
- Cognitive Linguistics
- Computational Linguistics
- Forensic Linguistics
- Grammar, Syntax and Morphology
- Historical and Diachronic Linguistics
- History of English
- Language Acquisition
- Language Evolution
- Language Reference
- Language Variation
- Language Families
- Lexicography
- Linguistic Anthropology
- Linguistic Theories
- Linguistic Typology
- Phonetics and Phonology
- Psycholinguistics
- Sociolinguistics
- Translation and Interpretation
- Writing Systems
- Browse content in Literature
- Bibliography
- Children's Literature Studies
- Literary Studies (Asian)
- Literary Studies (European)
- Literary Studies (Eco-criticism)
- Literary Studies (Romanticism)
- Literary Studies (American)
- Literary Studies (Modernism)
- Literary Studies - World
- Literary Studies (1500 to 1800)
- Literary Studies (19th Century)
- Literary Studies (20th Century onwards)
- Literary Studies (African American Literature)
- Literary Studies (British and Irish)
- Literary Studies (Early and Medieval)
- Literary Studies (Fiction, Novelists, and Prose Writers)
- Literary Studies (Gender Studies)
- Literary Studies (Graphic Novels)
- Literary Studies (History of the Book)
- Literary Studies (Plays and Playwrights)
- Literary Studies (Poetry and Poets)
- Literary Studies (Postcolonial Literature)
- Literary Studies (Queer Studies)
- Literary Studies (Science Fiction)
- Literary Studies (Travel Literature)
- Literary Studies (War Literature)
- Literary Studies (Women's Writing)
- Literary Theory and Cultural Studies
- Mythology and Folklore
- Shakespeare Studies and Criticism
- Browse content in Media Studies
- Browse content in Music
- Applied Music
- Dance and Music
- Ethics in Music
- Ethnomusicology
- Gender and Sexuality in Music
- Medicine and Music
- Music Cultures
- Music and Religion
- Music and Media
- Music and Culture
- Music Education and Pedagogy
- Music Theory and Analysis
- Musical Scores, Lyrics, and Libretti
- Musical Structures, Styles, and Techniques
- Musicology and Music History
- Performance Practice and Studies
- Race and Ethnicity in Music
- Sound Studies
- Browse content in Performing Arts
- Browse content in Philosophy
- Aesthetics and Philosophy of Art
- Epistemology
- Feminist Philosophy
- History of Western Philosophy
- Metaphysics
- Moral Philosophy
- Non-Western Philosophy
- Philosophy of Science
- Philosophy of Language
- Philosophy of Mind
- Philosophy of Perception
- Philosophy of Action
- Philosophy of Law
- Philosophy of Religion
- Philosophy of Mathematics and Logic
- Practical Ethics
- Social and Political Philosophy
- Browse content in Religion
- Biblical Studies
- Christianity
- East Asian Religions
- History of Religion
- Judaism and Jewish Studies
- Qumran Studies
- Religion and Education
- Religion and Health
- Religion and Politics
- Religion and Science
- Religion and Law
- Religion and Art, Literature, and Music
- Religious Studies
- Browse content in Society and Culture
- Cookery, Food, and Drink
- Cultural Studies
- Customs and Traditions
- Ethical Issues and Debates
- Hobbies, Games, Arts and Crafts
- Natural world, Country Life, and Pets
- Popular Beliefs and Controversial Knowledge
- Sports and Outdoor Recreation
- Technology and Society
- Travel and Holiday
- Visual Culture
- Browse content in Law
- Arbitration
- Browse content in Company and Commercial Law
- Commercial Law
- Company Law
- Browse content in Comparative Law
- Systems of Law
- Competition Law
- Browse content in Constitutional and Administrative Law
- Government Powers
- Judicial Review
- Local Government Law
- Military and Defence Law
- Parliamentary and Legislative Practice
- Construction Law
- Contract Law
- Browse content in Criminal Law
- Criminal Procedure
- Criminal Evidence Law
- Sentencing and Punishment
- Employment and Labour Law
- Environment and Energy Law
- Browse content in Financial Law
- Banking Law
- Insolvency Law
- History of Law
- Human Rights and Immigration
- Intellectual Property Law
- Browse content in International Law
- Private International Law and Conflict of Laws
- Public International Law
- IT and Communications Law
- Jurisprudence and Philosophy of Law
- Law and Politics
- Law and Society
- Browse content in Legal System and Practice
- Courts and Procedure
- Legal Skills and Practice
- Legal System - Costs and Funding
- Primary Sources of Law
- Regulation of Legal Profession
- Medical and Healthcare Law
- Browse content in Policing
- Criminal Investigation and Detection
- Police and Security Services
- Police Procedure and Law
- Police Regional Planning
- Browse content in Property Law
- Personal Property Law
- Restitution
- Study and Revision
- Terrorism and National Security Law
- Browse content in Trusts Law
- Wills and Probate or Succession
- Browse content in Medicine and Health
- Browse content in Allied Health Professions
- Arts Therapies
- Clinical Science
- Dietetics and Nutrition
- Occupational Therapy
- Operating Department Practice
- Physiotherapy
- Radiography
- Speech and Language Therapy
- Browse content in Anaesthetics
- General Anaesthesia
- Browse content in Clinical Medicine
- Acute Medicine
- Cardiovascular Medicine
- Clinical Genetics
- Clinical Pharmacology and Therapeutics
- Dermatology
- Endocrinology and Diabetes
- Gastroenterology
- Genito-urinary Medicine
- Geriatric Medicine
- Infectious Diseases
- Medical Toxicology
- Medical Oncology
- Pain Medicine
- Palliative Medicine
- Rehabilitation Medicine
- Respiratory Medicine and Pulmonology
- Rheumatology
- Sleep Medicine
- Sports and Exercise Medicine
- Clinical Neuroscience
- Community Medical Services
- Critical Care
- Emergency Medicine
- Forensic Medicine
- Haematology
- History of Medicine
- Browse content in Medical Dentistry
- Oral and Maxillofacial Surgery
- Paediatric Dentistry
- Restorative Dentistry and Orthodontics
- Surgical Dentistry
- Browse content in Medical Skills
- Clinical Skills
- Communication Skills
- Nursing Skills
- Surgical Skills
- Medical Ethics
- Medical Statistics and Methodology
- Browse content in Neurology
- Clinical Neurophysiology
- Neuropathology
- Nursing Studies
- Browse content in Obstetrics and Gynaecology
- Gynaecology
- Occupational Medicine
- Ophthalmology
- Otolaryngology (ENT)
- Browse content in Paediatrics
- Neonatology
- Browse content in Pathology
- Chemical Pathology
- Clinical Cytogenetics and Molecular Genetics
- Histopathology
- Medical Microbiology and Virology
- Patient Education and Information
- Browse content in Pharmacology
- Psychopharmacology
- Browse content in Popular Health
- Caring for Others
- Complementary and Alternative Medicine
- Self-help and Personal Development
- Browse content in Preclinical Medicine
- Cell Biology
- Molecular Biology and Genetics
- Reproduction, Growth and Development
- Primary Care
- Professional Development in Medicine
- Browse content in Psychiatry
- Addiction Medicine
- Child and Adolescent Psychiatry
- Forensic Psychiatry
- Learning Disabilities
- Old Age Psychiatry
- Psychotherapy
- Browse content in Public Health and Epidemiology
- Epidemiology
- Public Health
- Browse content in Radiology
- Clinical Radiology
- Interventional Radiology
- Nuclear Medicine
- Radiation Oncology
- Reproductive Medicine
- Browse content in Surgery
- Cardiothoracic Surgery
- Gastro-intestinal and Colorectal Surgery
- General Surgery
- Neurosurgery
- Paediatric Surgery
- Peri-operative Care
- Plastic and Reconstructive Surgery
- Surgical Oncology
- Transplant Surgery
- Trauma and Orthopaedic Surgery
- Vascular Surgery
- Browse content in Science and Mathematics
- Browse content in Biological Sciences
- Aquatic Biology
- Biochemistry
- Bioinformatics and Computational Biology
- Developmental Biology
- Ecology and Conservation
- Evolutionary Biology
- Genetics and Genomics
- Microbiology
- Molecular and Cell Biology
- Natural History
- Plant Sciences and Forestry
- Research Methods in Life Sciences
- Structural Biology
- Systems Biology
- Zoology and Animal Sciences
- Browse content in Chemistry
- Analytical Chemistry
- Computational Chemistry
- Crystallography
- Environmental Chemistry
- Industrial Chemistry
- Inorganic Chemistry
- Materials Chemistry
- Medicinal Chemistry
- Mineralogy and Gems
- Organic Chemistry
- Physical Chemistry
- Polymer Chemistry
- Study and Communication Skills in Chemistry
- Theoretical Chemistry
- Browse content in Computer Science
- Artificial Intelligence
- Computer Architecture and Logic Design
- Game Studies
- Human-Computer Interaction
- Mathematical Theory of Computation
- Programming Languages
- Software Engineering
- Systems Analysis and Design
- Virtual Reality
- Browse content in Computing
- Business Applications
- Computer Security
- Computer Games
- Computer Networking and Communications
- Digital Lifestyle
- Graphical and Digital Media Applications
- Operating Systems
- Browse content in Earth Sciences and Geography
- Atmospheric Sciences
- Environmental Geography
- Geology and the Lithosphere
- Maps and Map-making
- Meteorology and Climatology
- Oceanography and Hydrology
- Palaeontology
- Physical Geography and Topography
- Regional Geography
- Soil Science
- Urban Geography
- Browse content in Engineering and Technology
- Agriculture and Farming
- Biological Engineering
- Civil Engineering, Surveying, and Building
- Electronics and Communications Engineering
- Energy Technology
- Engineering (General)
- Environmental Science, Engineering, and Technology
- History of Engineering and Technology
- Mechanical Engineering and Materials
- Technology of Industrial Chemistry
- Transport Technology and Trades
- Browse content in Environmental Science
- Applied Ecology (Environmental Science)
- Conservation of the Environment (Environmental Science)
- Environmental Sustainability
- Environmentalist Thought and Ideology (Environmental Science)
- Management of Land and Natural Resources (Environmental Science)
- Natural Disasters (Environmental Science)
- Nuclear Issues (Environmental Science)
- Pollution and Threats to the Environment (Environmental Science)
- Social Impact of Environmental Issues (Environmental Science)
- History of Science and Technology
- Browse content in Materials Science
- Ceramics and Glasses
- Composite Materials
- Metals, Alloying, and Corrosion
- Nanotechnology
- Browse content in Mathematics
- Applied Mathematics
- Biomathematics and Statistics
- History of Mathematics
- Mathematical Education
- Mathematical Finance
- Mathematical Analysis
- Numerical and Computational Mathematics
- Probability and Statistics
- Pure Mathematics
- Browse content in Neuroscience
- Cognition and Behavioural Neuroscience
- Development of the Nervous System
- Disorders of the Nervous System
- History of Neuroscience
- Invertebrate Neurobiology
- Molecular and Cellular Systems
- Neuroendocrinology and Autonomic Nervous System
- Neuroscientific Techniques
- Sensory and Motor Systems
- Browse content in Physics
- Astronomy and Astrophysics
- Atomic, Molecular, and Optical Physics
- Biological and Medical Physics
- Classical Mechanics
- Computational Physics
- Condensed Matter Physics
- Electromagnetism, Optics, and Acoustics
- History of Physics
- Mathematical and Statistical Physics
- Measurement Science
- Nuclear Physics
- Particles and Fields
- Plasma Physics
- Quantum Physics
- Relativity and Gravitation
- Semiconductor and Mesoscopic Physics
- Browse content in Psychology
- Affective Sciences
- Clinical Psychology
- Cognitive Psychology
- Cognitive Neuroscience
- Criminal and Forensic Psychology
- Developmental Psychology
- Educational Psychology
- Evolutionary Psychology
- Health Psychology
- History and Systems in Psychology
- Music Psychology
- Neuropsychology
- Organizational Psychology
- Psychological Assessment and Testing
- Psychology of Human-Technology Interaction
- Psychology Professional Development and Training
- Research Methods in Psychology
- Social Psychology
- Browse content in Social Sciences
- Browse content in Anthropology
- Anthropology of Religion
- Human Evolution
- Medical Anthropology
- Physical Anthropology
- Regional Anthropology
- Social and Cultural Anthropology
- Theory and Practice of Anthropology
- Browse content in Business and Management
- Business Strategy
- Business Ethics
- Business History
- Business and Government
- Business and Technology
- Business and the Environment
- Comparative Management
- Corporate Governance
- Corporate Social Responsibility
- Entrepreneurship
- Health Management
- Human Resource Management
- Industrial and Employment Relations
- Industry Studies
- Information and Communication Technologies
- International Business
- Knowledge Management
- Management and Management Techniques
- Operations Management
- Organizational Theory and Behaviour
- Pensions and Pension Management
- Public and Nonprofit Management
- Social Issues in Business and Management
- Strategic Management
- Supply Chain Management
- Browse content in Criminology and Criminal Justice
- Criminal Justice
- Criminology
- Forms of Crime
- International and Comparative Criminology
- Youth Violence and Juvenile Justice
- Development Studies
- Browse content in Economics
- Agricultural, Environmental, and Natural Resource Economics
- Asian Economics
- Behavioural Finance
- Behavioural Economics and Neuroeconomics
- Econometrics and Mathematical Economics
- Economic Systems
- Economic History
- Economic Methodology
- Economic Development and Growth
- Financial Markets
- Financial Institutions and Services
- General Economics and Teaching
- Health, Education, and Welfare
- History of Economic Thought
- International Economics
- Labour and Demographic Economics
- Law and Economics
- Macroeconomics and Monetary Economics
- Microeconomics
- Public Economics
- Urban, Rural, and Regional Economics
- Welfare Economics
- Browse content in Education
- Adult Education and Continuous Learning
- Care and Counselling of Students
- Early Childhood and Elementary Education
- Educational Equipment and Technology
- Educational Strategies and Policy
- Higher and Further Education
- Organization and Management of Education
- Philosophy and Theory of Education
- Schools Studies
- Secondary Education
- Teaching of a Specific Subject
- Teaching of Specific Groups and Special Educational Needs
- Teaching Skills and Techniques
- Browse content in Environment
- Applied Ecology (Social Science)
- Climate Change
- Conservation of the Environment (Social Science)
- Environmentalist Thought and Ideology (Social Science)
- Management of Land and Natural Resources (Social Science)
- Natural Disasters (Environment)
- Pollution and Threats to the Environment (Social Science)
- Social Impact of Environmental Issues (Social Science)
- Sustainability
- Browse content in Human Geography
- Cultural Geography
- Economic Geography
- Political Geography
- Browse content in Interdisciplinary Studies
- Communication Studies
- Museums, Libraries, and Information Sciences
- Browse content in Politics
- African Politics
- Asian Politics
- Chinese Politics
- Comparative Politics
- Conflict Politics
- Elections and Electoral Studies
- Environmental Politics
- Ethnic Politics
- European Union
- Foreign Policy
- Gender and Politics
- Human Rights and Politics
- Indian Politics
- International Relations
- International Organization (Politics)
- Irish Politics
- Latin American Politics
- Middle Eastern Politics
- Political Methodology
- Political Communication
- Political Philosophy
- Political Sociology
- Political Behaviour
- Political Economy
- Political Institutions
- Political Theory
- Politics and Law
- Politics of Development
- Public Administration
- Public Policy
- Qualitative Political Methodology
- Quantitative Political Methodology
- Regional Political Studies
- Russian Politics
- Security Studies
- State and Local Government
- UK Politics
- US Politics
- Browse content in Regional and Area Studies
- African Studies
- Asian Studies
- East Asian Studies
- Japanese Studies
- Latin American Studies
- Middle Eastern Studies
- Native American Studies
- Scottish Studies
- Browse content in Research and Information
- Research Methods
- Browse content in Social Work
- Addictions and Substance Misuse
- Adoption and Fostering
- Care of the Elderly
- Child and Adolescent Social Work
- Couple and Family Social Work
- Direct Practice and Clinical Social Work
- Emergency Services
- Human Behaviour and the Social Environment
- International and Global Issues in Social Work
- Mental and Behavioural Health
- Social Justice and Human Rights
- Social Policy and Advocacy
- Social Work and Crime and Justice
- Social Work Macro Practice
- Social Work Practice Settings
- Social Work Research and Evidence-based Practice
- Welfare and Benefit Systems
- Browse content in Sociology
- Childhood Studies
- Community Development
- Comparative and Historical Sociology
- Disability Studies
- Economic Sociology
- Gender and Sexuality
- Gerontology and Ageing
- Health, Illness, and Medicine
- Marriage and the Family
- Migration Studies
- Occupations, Professions, and Work
- Organizations
- Population and Demography
- Race and Ethnicity
- Social Theory
- Social Movements and Social Change
- Social Research and Statistics
- Social Stratification, Inequality, and Mobility
- Sociology of Religion
- Sociology of Education
- Sport and Leisure
- Urban and Rural Studies
- Browse content in Warfare and Defence
- Defence Strategy, Planning, and Research
- Land Forces and Warfare
- Military Administration
- Military Life and Institutions
- Naval Forces and Warfare
- Other Warfare and Defence Issues
- Peace Studies and Conflict Resolution
- Weapons and Equipment

- < Previous chapter
- Next chapter >
8 Treatment of Social Anxiety Disorder: A Case Complicated by Panic Disorder
- Published: February 2013
- Cite Icon Cite
- Permissions Icon Permissions
Chapter 8 covers the treatment of Social Anxiety Disorder (SAD), and includes information about the condition, epidemiological considerations, the case study, assessment strategy and case formulation, intervention model and course of treatment, strategies for handling homework non-compliance, handling poor attendance and relapse, relapse prevention, post-treatment assessment, basic science for this case/condition, alternative strategies to consider, ethical consideration, cultural factors, clinical implications, and avoiding common mistakes during treatment.
Personal account
- Sign in with email/username & password
- Get email alerts
- Save searches
- Purchase content
- Activate your purchase/trial code
- Add your ORCID iD
Institutional access
Sign in with a library card.
- Sign in with username/password
- Recommend to your librarian
- Institutional account management
- Get help with access
Access to content on Oxford Academic is often provided through institutional subscriptions and purchases. If you are a member of an institution with an active account, you may be able to access content in one of the following ways:
IP based access
Typically, access is provided across an institutional network to a range of IP addresses. This authentication occurs automatically, and it is not possible to sign out of an IP authenticated account.
Choose this option to get remote access when outside your institution. Shibboleth/Open Athens technology is used to provide single sign-on between your institution’s website and Oxford Academic.
- Click Sign in through your institution.
- Select your institution from the list provided, which will take you to your institution's website to sign in.
- When on the institution site, please use the credentials provided by your institution. Do not use an Oxford Academic personal account.
- Following successful sign in, you will be returned to Oxford Academic.
If your institution is not listed or you cannot sign in to your institution’s website, please contact your librarian or administrator.
Enter your library card number to sign in. If you cannot sign in, please contact your librarian.
Society Members
Society member access to a journal is achieved in one of the following ways:
Sign in through society site
Many societies offer single sign-on between the society website and Oxford Academic. If you see ‘Sign in through society site’ in the sign in pane within a journal:
- Click Sign in through society site.
- When on the society site, please use the credentials provided by that society. Do not use an Oxford Academic personal account.
If you do not have a society account or have forgotten your username or password, please contact your society.
Sign in using a personal account
Some societies use Oxford Academic personal accounts to provide access to their members. See below.
A personal account can be used to get email alerts, save searches, purchase content, and activate subscriptions.
Some societies use Oxford Academic personal accounts to provide access to their members.
Viewing your signed in accounts
Click the account icon in the top right to:
- View your signed in personal account and access account management features.
- View the institutional accounts that are providing access.
Signed in but can't access content
Oxford Academic is home to a wide variety of products. The institutional subscription may not cover the content that you are trying to access. If you believe you should have access to that content, please contact your librarian.
For librarians and administrators, your personal account also provides access to institutional account management. Here you will find options to view and activate subscriptions, manage institutional settings and access options, access usage statistics, and more.
Our books are available by subscription or purchase to libraries and institutions.
| Month: | Total Views: |
|---|---|
| October 2022 | 3 |
| November 2022 | 2 |
| December 2022 | 3 |
| January 2023 | 2 |
| February 2023 | 4 |
| March 2023 | 4 |
| April 2023 | 1 |
| May 2023 | 1 |
| June 2023 | 2 |
| July 2023 | 2 |
| August 2023 | 2 |
| September 2023 | 6 |
| October 2023 | 3 |
| November 2023 | 3 |
| December 2023 | 3 |
| January 2024 | 3 |
| February 2024 | 1 |
| March 2024 | 3 |
| April 2024 | 4 |
| May 2024 | 7 |
| June 2024 | 4 |
| July 2024 | 1 |
- About Oxford Academic
- Publish journals with us
- University press partners
- What we publish
- New features
- Open access
- Rights and permissions
- Accessibility
- Advertising
- Media enquiries
- Oxford University Press
- Oxford Languages
- University of Oxford
Oxford University Press is a department of the University of Oxford. It furthers the University's objective of excellence in research, scholarship, and education by publishing worldwide
- Copyright © 2024 Oxford University Press
- Cookie settings
- Cookie policy
- Privacy policy
- Legal notice
This Feature Is Available To Subscribers Only
Sign In or Create an Account
This PDF is available to Subscribers Only
For full access to this pdf, sign in to an existing account, or purchase an annual subscription.
Sign up for your FREE e-newsletter
You’ll regularly recieve powerful strategies for personal development, tips to improve the growth of your counselling practice, the latest industry news and much more.
We’ll keep your information private and never sell, rent, trade or share it with any other organisation. And you can cancel anytime.
Counselling Case Study: Social Anxiety
Sasha is a 60 year old woman who has recently retired from a career in teaching. Working for many years in a secondary school environment, Sasha was confident, motivated and dedicated to her work, but at the same time looking forward to retirement so she and her husband could travel and spend more time with their adult children who lived nearby.
However upon finishing work, Sasha found herself experiencing severe anxiety, particularly when around other people, and began not wanting to leave the house or invite people into the house. She also experienced bouts of crying when attempting to complete tasks such as housework and using the sewing machine. Sasha found her symptoms eased when she and her husband went on camping trips in national parks where they often did not see other people for days.
While working with Sasha, the Professional Counsellor adopts strategies from Cognitive Behavioural Therapy and Gestalt frameworks in order to address any irrational thoughts and behaviours which may be maintaining Sasha’s anxiety, and to complete any unfinished business which may have led to the development of her anxieties in the first place. For ease of writing, the Professional Counsellor is abbreviated to “C”.
Sasha was an unplanned baby, born after her older brother. Her parents did not want a second child but when they realised another was on the way, they hoped for another boy. As a child Sasha remembers always being in the background and her brother and father being the ‘important’ ones.
Sasha reported a vivid memory of coming home from school one day and finding no-one home. Sasha sat on the front porch and cried until her mother eventually came home and told her to stop being so silly. She described her mother as being more concerned with the state of the house than with her young daughter.
Sasha’s father died when she was very young, and she remembers her mother not coping well for a long time. During this time she (but not her brother) was often sent to her grandparents’ farm to give her mother a break. Here Sasha spent most days on her own. However she remembers these visits fondly, like ‘a lull in the storm’.
When her mother died, she left everything to Sasha’s brother, who was by then a well- paid solicitor with a young family. Sasha also had a young family but did not question her mother’s decision as she had been conditioned from childhood to believe males were more important.
Issues identified
Sasha’s symptoms appeared to be those of social anxiety disorder. They included:
- An extreme fear of situations where she may have to meet new people or be scrutinized by others.
- Social situations were either experienced with intense anxiety or avoided altogether.
When she did face these situations, she experienced physical symptoms such as sweating, shaking, tension, shaky voice, dry mouth and a pounding heart. The main symptom of this disorder involves feeling extreme anxiety in the presence of others. Sufferers often believe other people are very confident in public and that they are the only ones who aren’t.
Almost everyone experiences some social anxiety now and then; however social anxiety disorder severely limits the lifestyle of the sufferer, causing them to avoid making friends or miss important opportunities at work.
Formulation
In the first session, Sasha described her current physical symptoms and her feelings of hopelessness that she would never have the lifestyle she had dreamed of having in retirement. She was very tearful and her voice was quite high and shaky. She stuttered occasionally and her hands moved constantly, tearing the tissue she was holding to pieces.
She described trying to sew curtains and being overtaken by an uncontrollable fit of crying. She could not explain why this had made her so upset. She had also avoided inviting former work colleagues to her house for fear it would not be ‘good enough’. Her main concern was her daughter’s wedding, coming up in three months. She became more tearful talking about this, saying she did not know how the bride’s mother was supposed to look or act.
C then took a history of Sasha’s family background and noted that she had always been relegated to the background, leading to the core belief that she was unimportant. Sasha then described her work history which seemed to be in sharp contrast to her family experiences. C took some time to explore this with Sasha.
Sasha described being in the classroom as ‘being in control’. She felt that she had a good rapport with students and was good at her job. She often took on more than she could handle at work but somehow managed to get through it and was praised by her colleagues when she did this. It appeared that the only time Sasha had ever felt important was in the workplace.
However while she got along with other staff, she had made no real friends and had never had any friends throughout her life. C asked her why this was. Sasha became tearful again and said that she just wanted to go and live somewhere she wouldn’t have to see anyone except her husband and her children. She described her camping trips with her husband as being relaxed because she didn’t have to talk to other people. She experienced particular anxiety when her husband’s family visited as she felt pressure to be a perfect wife and housekeeper in their eyes.
Sasha mentioned that while she was working in the Education Department, she had been given a personality test to complete which had told her she was an extrovert. She was puzzled by this because she did not like people and clearly stated that it was not her goal in counselling to change this.
At this stage, C shared with Sasha her impression that Sasha appeared to have developed the belief that her authentic self was unacceptable and had created a false self to present to the world. This created intense anxiety because she was never quite sure who people wanted her to be from one situation to the next, requiring her to constantly scan her environment for clues as to how to feel and behave. Consequently it was easier to think about going away to a place where she would not have to see anyone, as she had done as a child at her grandparents’ farm. Only when she was away from people was she able to relax and feel in control.
Also, because she had married an introverted man who indulged her need to avoid social situations, she had learned to suppress her extroverted nature still further. It was no surprise that retirement was causing her such distress, since the only time she had ever felt important and comfortable around people had been in the work environment.
Session Content
Empty chair.
C decided to explore the unexpressed extroverted side of Sasha’s personality first. She asked Sasha what she did that was fun. Sasha could only list one item, the morning walk she took with her husband in the hills. Even this caused her concern however, because she felt she should be walking faster and further than she was.
Using the Gestalt technique known as Empty Chair, C placed a chair opposite Sasha and asked her if she would speak to the extroverted side of herself. Sasha found it difficult to stay in the first person and avoided this by talking directly to C. C guided her attention back to the empty chair and suggested she ask this part of herself what it would do if it could take over for a day.
When Sasha had done this, C asked her to move to the empty chair and reply as her extroverted self. Once seated in the other chair, Sasha began to relax and freely spoke about wanting to go to Dreamworld and wanting to make a quilt. When she returned to her original seat, C asked Sasha how she felt about allowing this side of her to have some fun. Sasha appeared reluctant but agreed to ask her husband if he would go to Dreamworld with her.
In the following session, Sasha reported she had not only gone to Dreamworld, but that they had purchased season tickets. Throughout the course of the counselling sessions, Sasha and her husband began visiting the theme park for half a day every week. She also started several creative projects, including hand quilting and scrap booking. She found these activities extremely difficult at first, but utilising cognitive-behavioural strategies to challenge her core beliefs, she was able to continue to the point where she was able to enjoy herself for the first time in years.
Cognitive Restructuring
Challenging and modifying a client’s faulty thought processes is the basis of Cognitive Behavioural Therapy (CBT). After Sasha had outlined several situations that were causing her anxiety, C helped her identify her beliefs about these situations. Sasha was shown that it was her beliefs about these situations which led to her bad feelings, and was encouraged to find more realistic alternative beliefs. Some of these processes included:
Activating event (A) = sewing
Belief (B) = I can’t do it well enough, I might as well give up
Consequence (C) = crying, giving up, bored and depressed
Dispute (D) = I’ll do my best and focus on enjoying myself rather than focusing on the outcome
A = husband’s family staying
B = they’ll see the state of my house and be horrified
D = I’ve got better things to do than clean the house and if they don’t like it, it doesn’t mean I’m a bad wife
A = attending daughter’s wedding
B = I’ll let her down and embarrass the whole family by saying or doing something wrong
D = people will be focusing on the bride, not me, so I’ll focus on her too
In this manner, Sasha was asked to practice disputing her thoughts for homework.
C then asked Sasha to use the Empty Chair technique to complete unfinished business with her mother, addressing her feelings about coming home to an empty house and then being told she was ‘silly’ for crying. Sasha had always believed her mother had treated her as insignificant because she had been such an inadequate child. Playing both roles, Sasha was able to see that her mother had her own agenda which made it difficult for her to have time for her daughter. After Sasha told her mother via the Empty Chair technique how she had felt in this situation, she realised the beliefs she had developed about herself were not necessarily accurate or helpful and could therefore be challenged.
Again reverting to CBT techniques, C asked Sasha to look for disconfirming evidence for the belief that she was inadequate. She was able to find many examples of this, chiefly in her work and as a mother to her own children. Sasha was asked to continue noticing examples like this on a daily basis. She was also asked to be aware of herself in the present moment as much as possible, rather than focusing on the past or the future. This allowed her to enjoy what she was doing, rather than focusing on previous failures and criticisms, or future ‘what ifs’.
Session Summary
Sasha’s counselling sessions focused on a number of issues:
- Integrating repressed parts of herself that were ‘unacceptable’
- Allowing her extroverted side to be expressed so she could take part in and enjoy pleasurable activities which lifted her depression
- Completing unfinished business with her mother
- Challenging her thoughts and behaviours – the belief that she was unimportant and the need to compensate by being perfect
- Learning to be present in the here and now, allowing her to focus on the activity at hand and enjoy it, rather than worrying about the outcome Experimenting with relaxing her perfectionist standards, which showed her that nobody else even noticed.
- Her daughter’s wedding – Sasha discovered that by distracting her thoughts about being around so many other people in such an important role at her daughter’s wedding, and instead focusing on the needs of her daughter and guests, her anxiety was no longer present.
Sasha’s experiments reinforced the fact that her thoughts were producing her anxiety, not other people. She realised that when she wasn’t focused on herself, her anxiety was no longer there. When she couldn’t distract her thoughts, she learned to modify them to something more realistic. By challenging her irrational belief that if she wasn’t perfect she was inadequate, she began to enjoy everyday activities and became much more relaxed. This was noticeable even in her voice, which lowered in tone, and in her generally more relaxed nonverbal behaviour.
As a result of implementing these strategies, Sasha found it a lot easier to be around other people. By learning to accept herself as she was, she no longer felt the need to guess what other people wanted from her, and began to feel comfortable presenting her authentic self to the world.
Author: Leanne Chapman is a Psychologist who has worked in community clinics and hospital settings with both children and adults. She has also conducted group therapy for patients with anxiety, depression and eating disorders at New Farm Clinic. In addition to her work with AIPC, Leanne operates a successful private practice.
- February 11, 2008
- Anxiety , Case Study , CBT , Gestalt , Stress
- Case Studies , Clinical Mental Health , Stress Management

Comments: 1

I found this article useful especially as it illustrates how effective forms of CBT can be in regard to treating anxiety. I thought the model used (ABC of Emotional Disturbance) was Albert Ellis’ Rational Emotive Behaviour Therapy. I think CBT and the ABC of Emotional Disturbance is sometimes attributed to the work of Beck and others. I have always understood that this was Ellis’ creation.
Thanks again for a very helpful article.
Leave a Reply Cancel reply
Your email address will not be published. Required fields are marked *
Case Study: Overcoming Anxiety – Success Stories

In this article
Anxiety is a formidable adversary in the everyday life of many people in the UK. According to statistics, around 6% of people are diagnosed with generalised anxiety disorder (GAD) every week and, in total, more than 8 million people experience an anxiety disorder. Characterised by excessive apprehension, worry and fear, anxiety comes in many forms. Generalised anxiety disorder is a persistent and excessive worry about everyday events. Social anxiety disorder , however, focuses on overwhelming fears of social situations. There are also several other disorders with anxiety-based symptoms. These include panic disorder, specific phobias , obsessive-compulsive disorder ( OCD ), post-traumatic stress disorder ( PTSD ), selective mutism and separation anxiety disorder. In this article, we’ll explore three case studies on people with different anxiety problems and how they overcame them.
Case Study 1: Overcoming Social Anxiety
Meet Sarah*, a 28-year-old professional who, for years, grappled with the debilitating effects of social anxiety disorder. Sarah’s anxiety manifested itself in a fear of social interactions. Since this problem crept up over time, Sarah didn’t realise how much of a problem she had until her early 20s when she left university and began working in her professional field. Ultimately, Sarah recognised she had a problem that others didn’t seem to have, and it left her isolated and hindered in both her personal life and professional sphere.
Sarah’s social anxiety manifested itself in her avoidance of social events and gatherings. In work meetings she couldn’t avoid, she would feel sick, lightheaded and extremely nervous. She chose not to socialise with her colleagues and found it difficult to maintain friendships with more outgoing people. The most profound symptom for Sarah was her intense fear of being scrutinised and criticised. These intense emotions took their toll on her self-esteem. Recognising the need for change, Sarah began to explore her feelings and sought help.
Sarah knew there was no quick fix. Anxiety was something she’d lived with her entire life and she’d managed to mask her issues quite well. Her transformation began with her seeking the guidance of a mental health professional. After speaking initially with her GP, Sarah began a course of cognitive-behavioural therapy ( CBT ) where she gained valuable insights into the irrational thought patterns that were fuelling her anxiety. CBT equipped her with practical tools to challenge and reframe her thoughts. Gradually, these tools helped her to diminish the power anxiety held over her in specific situations.
At the same time, Sarah engaged in exposure therapy. This therapeutic approach introduced her gradually to situations that ordinarily would cause her immense fear. However, this systematic desensitisation process was done in a controlled and supportive environment, which allowed her to confront her anxieties gradually. Over time, Sarah was able to build up her resilience and confidence in these situations.
Beyond therapy and with the advice of an online support group, Sarah adopted mindfulness practices. She incorporated meditation and deep breathing into her daily routine. These mindfulness practice techniques became invaluable to her and helped her stay present and manage anxious thoughts during social interactions.
Sarah also took it upon herself to make lifestyle changes to promote good mental wellbeing. She began exercising routinely rather than sporadically as she had done before and noticed improvements in mood and a reduction in stress.
Through consistent effort, Sarah emerged triumphant over her social anxiety. Today, she is able to deal with social situations much more easily than before. She can handle new situations well, both professionally and personally, while acknowledging that she’ll always have a tendency to feel anxious and will need to continue practising techniques that she now knows work.
Sarah’s story underscores the effectiveness of tailored therapeutic interventions and lifestyle adjustments. Sarah remained committed and open-minded about the route she was taking. Though she chose not to try medication, she recognised that this was available to her if her chosen pathway didn’t have the desired effects she was looking for. Her journey serves as an inspiration for others dealing with similar struggles who are perhaps fearful of turning to medication.

Case Study 2: Triumphing Over Panic Attacks
Alex,* a 35-year-old plumber from Barnsley in South Yorkshire, struggled with the debilitating impact of frequent panic attacks for a number of years. Alex’s initial experiences with panic attacks occurred suddenly and intensely. He had recently undergone a series of major life changes, including a job promotion that came with increased responsibilities and higher expectations. Though he was excited and enthusiastic about the professional growth, the added pressure triggered heightened stress levels. Simultaneously, there were changes in his personal life. He’d just become a father for the first time and his child had had to spend several weeks in the NICU.
The combination of stressors, both professional and personal, created a perfect storm for anxiety. The pressure to excel in a new job while adapting to fatherhood and an ill baby became overwhelming for Alex. The first panic attack occurred just after a particularly stressful work meeting during which his wife, who was at the NICU with their baby, had called his mobile several times. After the initial panic attack, a cycle of anxiety and panic attacks began.
Alex’s initial experiences of panic attacks were characterised by sudden and intense episodes of fear, shortness of breath and dizziness. These attacks had a huge impact on various aspects of Alex’s life, causing disruptions in his work life and personal relationships.
Recognising the severity of the situation and needing to be strong for his wife and baby, Alex took the crucial step of seeking professional help. Alex was diagnosed with panic disorder, after which he began a course of treatment. Alex began cognitive-behavioural therapy as well as medication.
Alex’s therapist worked with him to develop coping strategies that empowered him to overcome the triggers to his panic attacks. His anti-anxiety medication and antidepressants helped Alex in the initial stages of treating his disorder to alleviate the frequency and intensity of his panic attacks.
On a personal level, Alex began ensuring he looked after himself through sufficient sleep, regular exercise and a healthier diet. Over time, Alex was able to come off his medication and, with continuing techniques learned in CBT, began living a life free from panic attacks once again.
Case Study 3: Mastering Generalised Anxiety
Chris’s*experiences with GAD were characterised by a constant state of worry and apprehension about various aspects of his life, from school performances to personal relationships. The generalised nature of the anxiety made it difficult for him to understand specific triggers, which led to a pervasive sense of unease and heightened stress levels.
After opening up to his parents, Chris saw his GP who offered him support through CBT. He also had support from his sixth-form college.
Chris’s CBT therapist helped him to see and challenge the maladaptive thought patterns he had. Through a series of structured sessions, Chris learned to identify and reframe irrational thoughts to gain a more balanced perspective on perceived threats. CBT provided Chris with practical tools and coping strategies that empowered him to manage situations that caused him anxiety.
At college, Chris joined a mindfulness group to learn techniques like meditation and relaxation. This helped him to reduce how often he wound up ruminating on future uncertainties. After committing to therapy and working hard to manage his anxiety, Chris became much more resilient.
Chris’s journey highlights the effectiveness of evidence-based interventions like CBT and mindfulness techniques in managing GAD. By addressing both the cognitive and emotional aspects of the disorder, people with GAD can form adaptive coping mechanisms to regain control over their lives.
Common Themes and Strategies
As we explore the diverse narratives of triumph over anxiety, several common themes emerge. Key among these is the importance of seeking support. Be it friends, family or mental health professionals, it is one of the most important principles that contribute to successful recovery.
Recognition and acknowledgement
In each case study, the individuals were all the first people to recognise and acknowledge that things weren’t right. This critical self-awareness marked the initial step to seeking help and initiating recovery. Acknowledging that things weren’t right allowed them to confront their issues and consider the possibility of—and hope for—positive change.
Professional guidance
All three individuals in our case studies recognised the importance of seeking professional help. Mental health professionals played an important role in their recoveries, providing tailored interventions like CBT and medication. Therapeutic relationships provide a safe space for exploration, understanding and the development of coping strategies.
Holistic approaches
A holistic approach to mental wellbeing in addition to professional interventions was key here too. Lifestyle changes like mindfulness practice, regular exercise and healthy diets were integral to their improvement.
Support systems
The support of friends and family is important too. Whether it was Sarah navigating social situations, Alex overcoming panic attacks or Chris managing his generalised anxiety at college, the presence of a supportive network was important. Open communication, understanding and empathy from loved ones create an environment that is conducive to recovery.
Coping mechanisms
Developing coping mechanisms was also integral to all three people’s recoveries. Each individual engaged in techniques tailored to their specific anxiety disorders. Exposure therapy can help with some phobias and social anxiety, whereas CBT can work with all forms of anxiety.
Persistence and commitment
Persistence and commitment are required to overcome anxiety, which is what makes this condition so tricky to manage. It’s a journey that takes a long time and there may be many bumps in the road on the way.

The Role of Resilience
One recurring theme stands out in all three case studies: resilience. Resilience is often defined as the ability to bounce back from adversity. Building resilience plays a huge role in any person’s journey to overcoming an anxiety disorder. It’s important to know that setbacks will happen and that this is natural and inevitable.
Navigating setbacks
Whether it’s facing initial discomfort or experiencing a panic attack after treatment has started, setbacks are an important part of the recovery process. Resilience means continuing to try despite the setback.
Learning and growth
Resilience enables you to see and approach a setback as an opportunity for learning and growth. Setbacks are not indicative of failure; they represent moments of refinement. They allow individuals to refine their coping mechanisms and build emotional strength.
Celebrating progress
Resilience isn’t just about getting through a tough time; it’s about celebrating progress. Recognising and acknowledging achievements, whether this is overcoming a fear or working well with coping strategies, reinforces the process.
Inspiring Others
The power of real-life success stories shows others who are about to start their journey or who have just started, that it is possible to get better. Sharing success stories is a beacon of hope for others. What’s more, openness is key to breaking the stigma that surrounds mental health. It shows that anxiety disorders can affect anyone, and that seeking help is not a sign of weakness but a courageous step towards a better future.
Real-life stories make the journey more tangible for individuals currently struggling with anxiety. Knowing that others have walked similar paths and come through the other side is positive. It instils a sense of optimism and motivation. Success stories also help to validate experiences. They make individuals feel less alone and isolated, showing that their conditions are legitimate and worthy of space.
Ultimately, case studies like Sarah’s, Alex’s and Chris’s serve as catalysts. They highlight the transformations that are possible, thus motivating individuals to take the first steps themselves.
Key Takeaways:
- Professional support matters: seeking professional help is a crucial step in the recovery process. Therapies like CBT and medication play a pivotal role.
- See the problem holistically: approach your mental wellbeing from a holistic perspective. Make lifestyle changes and seek social support.
- See resilience as a pillar: resilience is a key factor in recovery. Acknowledge setbacks, learn from them, and celebrate progress.
- Success is possible: through commitment, resilience and a combination of strategies, triumph over anxiety is an achievable reality.
*names have been changed

Anxiety Awareness
Study online and gain a full CPD certificate posted out to you the very next working day.
Take a look at this course
About the author

Louise Woffindin
Louise is a writer and translator from Sheffield. Before turning to writing, she worked as a secondary school language teacher. Outside of work, she is a keen runner and also enjoys reading and walking her dog Chaos.
Similar posts

Best Practices for Storing and Managing Student Records Securely

Recognising the Early Signs of Dyslexia in Children

Techniques for Supporting Loved Ones Battling Depression

Strategies for Parents Coping with the Loss of a Child
Celebrating our clients and partners.


An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- Indian J Psychol Med
- v.41(3); May-Jun 2019
A Case Report of Psychotic Symptoms in Social Anxiety Disorder
Gitanjali natarajan.
Department of Clinical Psychology, Amrita Institute of Medical Sciences, Kochi, Kerala, India
Sangeetha P. Louis
Praveen arathil.
1 Department of Psychiatry, Amrita Institute of Medical Sciences, Kochi, Kerala, India
Social phobias come under the category of phobic anxiety disorders and are centered around a fear of scrutiny by other people, usually leading to avoidance of social situations.[ 1 ] Although social anxiety has been found to be the most common comorbidity in people with psychosis,[ 2 ] social phobia or anxiety per se is a neurotic disorder in which the patient usually maintains an adequate touch with reality and is rarely associated with psychotic symptoms, beyond the self-referential feelings often observed in social anxiety disorder (SAD). Although there are a few contradictory pieces of evidence of the presence of psychotic symptoms in anxiety disorders,[ 3 , 4 ] it is usually accepted that there are clear lines of demarcation between anxiety disorders and psychosis. The exact prevalence of psychotic symptoms in SAD is not known. Although the presence of psychotic symptoms in SAD would have an immense impact on the severity, management, and prognosis of the disorder, there are only case reports available and the matter is not yet studied in a systematic manner. This case report details how a person with SAD gradually developed disorder-congruent delusions.
CASE REPORT
A 34-year-old married male, graduate in business administration, working as a clerical staff in the Middle East, premorbidly having anxious avoidant personality, presented to the clinical psychology department with a 3 years history of gradual onset of fear of blushing when meeting people and avoiding social interactions with familiar people, especially those in authority, after he started working in a new office. He had less anxiety when meeting unfamiliar people. His social phobia and avoidance increased in the last 2 years, with social interactions getting restricted to only his wife and child as well as colleagues during office work. He started avoiding phone conversations with friends and extended family members, as he believed that they would notice the change in his voice and come to know about his discomfort.
For the last 6 months, he started believing that his blushing during social interactions is offensive to others in the office. Moreover, he was convinced that his “fear of blushing” was contagious and was being transmitted to other people. He reported that he had transmitted his blushing to his supervisor who also started blushing during social encounters. He also believed that his supervisor was offended by the patient's presence, as he would blush more. Hence, the patient has been avoiding meeting his supervisor. Off late, he felt that more people in the office were finding him offensive, and he was transmitting the blushing to all of them. He wanted to stop going to the office, as he felt responsible for others’ discomfort. He returned to Kerala to get his problem treated.
There is no history suggestive of severe depression, as the patient did not have marked anhedonia, fatigue, or diminished activity. He had past history of low mood, feeling tired, and increase in sleep and appetite that persisted for a few months after he failed in his pre-degree examination 18 years back and it resolved without treatment. Family history of depression in paternal uncle, personal history of restrictive upbringing by parents, and premorbid anxious-avoidant traits were reported. Mental status examination showed low mood, worries about his social anxiety, and firm belief about others finding him offensive as he was transmitting “fear of blushing” to them. He admitted to the possibility that there could be something wrong in his mind, and hence, wanted treatment.
A detailed psycho-diagnostic assessment indicated average intellectual functioning, social anxiety, depressive symptoms, and a high tendency for fantasy. On Beck Depression Inventory scale, he got a score of 26 indicating moderate depressive symptoms; on Beck Anxiety Inventory scale, a score of 16 indicating mild anxiety symptoms; and on Social Interaction Anxiety scale, a score of 43 indicating presence of social anxiety disorder. The diagnosis of SAD was retained as the client did not fit the criteria for severe depression with psychotic symptoms or persistent delusional disorder.
Management involved a combination of paroxetine controlled release tablets and cognitive behavior therapy (CBT) involving cue-controlled relaxation, graded exposure, and cognitive restructuring. At 1 year follow-up, the patient still continued having the delusion that his boss had developed social anxiety and blushing through him, but it appeared to have become encapsulated and to be not interfering in his daily functioning in the office. He continued interacting with his boss through phone whenever possible. He no longer believed that he was transmitting social anxiety to all his colleagues. His interaction with colleagues was normal, and he was no longer reluctant to go to his office.
This case is different from a typical case of social phobia in two aspects: first by the presence of a firm belief that his symptoms of social anxiety, especially his fear of blushing, were contagious and his concern over spreading this fear to more and more people, and second, by his conviction that others found his social discomfort offensive.
The false belief in this patient is similar to the offensive subtype of Taijin-Kyofusho (TKS), a condition mentioned under SAD in Diagnostic and Statistical Manual of Mental Disorders 5.[ 5 ] The offensive subtype of TKS includes patients with a delusional conviction of offensiveness-persistent and excessive fear of causing offence to others in social circumstances by physical characteristics such as blushing, facial expressions, body odors, or intestinal noises. Cultural and societal norms engendering guilt, shame, and embarrassment are also likely etiological factors.[ 6 ] Belonging to a collective society with restricted upbringing, the patient would be more attentive and sensitive to the thoughts, feelings, and behaviors of significant others.
Three explanations have been suggested for the psychotic manifestations in SAD: (1) the individual's inability to challenge his social fears; (2) stressor and perpetuating role of SAD; and (3) the possibility of a primary thought abnormality leading to psychotic self-reference.[ 3 ] Greater paranoid ideation, in a non-clinical sample, was found to be associated with higher levels of social anxiety, avoidance, apprehension about evaluation, self-observation, and low self-esteem.[ 7 ]
The transformation of social apprehensions to a delusional level could also be explained using the changes in “social brain” and perception because of the increasingly worsening social isolation.[ 8 , 9 ] This could explain how the patient's initial fears of blushing and discomfort progressed into a delusional level with increasing isolation.
The patient improved with treatment focused on SAD - using Selective Serotonin Reuptake Inhibitor and CBT. Antipsychotics have been found to have a lower efficacy in SAD even when delusions are present. This may be because of the hypoactivity of dopaminergic circuits and D2 receptor found in SAD. Antipsychotics could further reduce dopamine action in a system that is already in deficit.[ 3 ]
The above case highlights that the commonly assumed demarcation between anxiety disorders and psychosis is questionable and points to the fragility of current diagnostic constructs. Affective and psychotic phenomena often co-occur, and such a co-occurrence predicts a poorer course and outcome, with greater persistence of schizotypal and negative symptoms, more illness behavior, greater likelihood of service use, and more evidence of familial liability for mental illness.[ 4 ] New diagnostic subcategories or expanding the social anxiety diagnosis to include psychotic symptoms, as in mood disorders, would have to be considered. This case also suggests that SAD with psychosis could be an entity midway in the dimensional spectrum between SAD and delusional disorder. In addition, the role of social isolation, secondary to social phobia, in the development of psychotic symptoms among patients with social phobia also needs to be further explored.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Conflicts of interest.
There are no conflicts of interest.
Very early family-based intervention for anxiety: two case studies with toddlers

Aude Henin ,
Stephanie J Rapoport ,
Timothy E Wilens ,
Alice S Carter .
https://doi.org/ 10.1136/gpsych-2019-100156
Anxiety disorders represent the most common category of psychiatric disorder in children and adolescents and contribute to distress, impairment and dysfunction. Anxiety disorders or their temperamental precursors are often evident in early childhood, and anxiety can impair functioning, even during preschool age and in toddlerhood. A growing number of investigators have shown that anxiety in preschoolers can be treated efficaciously using cognitive–behavioural therapy (CBT) administered either by training the parents to apply CBT strategies with their children or through direct intervention with parents and children. To date, most investigators have drawn the line at offering direct CBT to children under the age of 4. However, since toddlers can also present with impairing symptoms, and since behaviour strategies can be applied in older preschoolers with poor language ability successfully, it ought to be possible to apply CBT for anxiety to younger children as well. We therefore present two cases of very young children with impairing anxiety (ages 26 and 35 months) and illustrate the combination of parent-only and parent–child CBT sessions that comprised their treatment. The treatment was well tolerated by parents and children and showed promise for reducing anxiety symptoms and improving coping skills.
- Introduction
Anxiety disorders affect as many as 30% of children and adolescents and contribute to social and academic dysfunction. These disorders or their temperamental precursors 1 are often evident in early childhood, with 10% of children ages 2–5 already exhibiting anxiety disorders. 2 Anxiety symptoms in toddlerhood 3 and preschool age 4 show moderate persistence and map on to the corresponding Diagnostic and Statistic Manual anxiety disorders. 5 6 Well-meaning parents, particularly those with anxiety disorders themselves, may respond to a child’s distress around separating from parents or being around unfamiliar children by decreasing the child’s exposure to these situations, for example, by not having the child start preschool or by not leaving the child with a childcare provider to go to work or socialise. In the short term, such responses may impair concurrent family function, strain the parent–child relationship, and reduce the child’s opportunity for increased autonomy, learning and social development. 7 These avoidant strategies may initiate a trajectory where the child takes part in fewer and fewer activities, leading to social and academic dysfunction. 8
Members of our research team began championing the idea of early intervention with young anxious children over two decades ago, with the aim of teaching children and their parents cognitive–behavioural strategies to manage anxiety before their symptoms became too debilitating. 8 Although cognitive–behavioural therapy (CBT) has since emerged as the psychosocial treatment of choice for treating and preventing anxiety, 9 10 at that time, most protocols that had been empirically tested were aimed at children ages 7 through early adolescence, with only a few enrolling children as young as age 6. 11 We developed and tested a parent–child CBT intervention (called ‘Being Brave’) and reported efficacy in children as young as 4 years. 12 13 The treatment involved teaching parents about fostering adaptive coping and implementing graduated exposures to feared situations, and modelling how to teach children basic coping skills and conduct exposures with reinforcement. In parallel, a growing number of investigators confirmed that anxiety in preschoolers could be treated efficaciously using CBT administered either by training parents to apply CBT strategies with their children or through direct intervention with children. 14 15 Early family-based intervention using cognitive–behavioural strategies was shown to reduce rates of later anxiety and to attenuate the onset of depression in adolescence in girls. 16
The question remains as to whether early intervention can be extended even younger. With few exceptions, 17 18 most investigators do not offer direct CBT for anxiety to children under age 3 or 4, 15 and none to our knowledge have treated anxiety disorders with CBT in children under age 2.7. 15 However, we reasoned that since toddlers can also present with impairing symptoms, and since behaviour strategies can be feasibly applied even in preschoolers with poor language ability, 19 it ought to be possible to apply family-based CBT for anxiety to toddlers as well. We therefore present two cases of anxious children, ages 26 and 35 months, treated with parent and child CBT.
Recruitment
Parents of children ages 21–35 months were recruited for a pilot intervention study (a maximum of three cases) using advertisements to the community. To be included, children had to be rated by a parent as above a standard deviation on the Early Childhood Behavior Questionnaire Fear or Shyness Scale 20 and could not have global developmental delays, autism spectrum disorder or a primary psychiatric disorder other than anxiety.
Children were evaluated for behavioural inhibition using a 45 min observational protocol. 21 Parents completed a structured diagnostic interview about the child (Kiddie Schedule for Affective Disorders and Schizophrenia-Present and Lifetime) that has been used with parents of children as young as 2 years; 22 23 an adapted Coping Questionnaire, 24 in which parents assessed the child’s ability to cope with their six most feared situations; and questionnaires assessing child symptoms (Child Behavior Checklist 1-1/2-5 (CBCL), 25 subscales from the Infant Toddler Social Emotional Assessment (ITSEA) 26 ), family function (Family Life Impairment Scale 27 ) and parental stress (Depression Anxiety Stress Scale 28 ). These assessments were repeated following the intervention, with the exception of the behavioural observation for the child initially rated ‘not inhibited’. The clinician rated the global severity of the child’s anxiety on a 7-point severity scale (Clinician Global Impression of Anxiety 29 ) at baseline and rated global severity and improvement of anxiety postintervention. Participant engagement in session and adherence to between-session assignments were rated by the clinician at each visit, and parents completed a post-treatment questionnaire rating the intervention.
Children were treated by the first author, a licensed child psychologist, using the ‘Being Brave’ programme. 13 It includes six parent-only sessions, eight or more parent–child sessions and a final parent-only session on relapse prevention. An accompanying parent workbook reinforces the information presented. Parent-only sessions focus on factors maintaining anxiety; monitoring the child’s anxious responses and their antecedents and consequences; restructuring parents’ anxious thoughts; identifying helpful/unhelpful responses to child anxiety; modelling adaptive coping; playing with the child in a non-directive way; protecting the child from danger rather than anxiety; using praise to reinforce adaptive coping; and planning and implementing graduated exposure. Child–parent sessions teach the child basic coping skills; and focus on planning, rehearsing and performing exposure exercises, often introduced as games, with immediate reinforcement. All parent–child sessions were preserved from the original protocol, but two sessions teaching the child about the CBT model, relaxation and coping plans were omitted, as were two sessions in which the (older) child does a summary project and celebrates gains. Up to six child–parent sessions focusing on exposure practice were included.
In the cases that follow, identifying details are disguised to protect participants’ privacy. Parents of both children provided written consent for the publication of de-identified case reports.
Background information
‘J’ was a 35-month-old girl, the third of three children of married parents. She had congenital medical problems requiring multiple surgeries, and she continued to undergo regular follow-up procedures. J met the criteria for separation anxiety disorder with marked severity, mild social phobia and mild specific phobia. Although she was able to attend her familiar day care if handed directly to a teacher and attend a gymnastics class with a friend while her mother waited in the hall, J showed great distress if apart from her mother at home. If her mother left her sight (eg, to use the bathroom), J would sob, cry and try to open the door to get in. If her mother went out and left her with a family member, J would fuss, cry and try to come along, and would continually ask to video-call her, so her mother would cut her outings short. J also had fears of doctors’ visits, of riding in the car seat, and of walking independently up and down a staircase at home. She would approach new children only with assistance from her mother, and she was afraid to take part in gymnastics performances.
J also had some mood symptoms possibly related to her medical issues. She would intermittently have days when she was much more clingy, had uncharacteristically low energy, would want to be held, and would say ‘ow, ow’ if put down to stand. She also had difficulty staying asleep and would periodically wake up with respiratory difficulties.
‘K’ was a 26-month-old boy, the only child of married parents. He met the criteria for moderate separation anxiety disorder. Although able to go to a day care he had been attending since infancy, he showed distress at drop-off particularly at the start of each week, crying for 15 min. He feared being apart from his mother in the house: he could not tolerate his mother leaving the room even to change clothes and would cry if his mother left the playroom while K played with his father. He would get distressed if his father took him on outings without his mother. He could not be dropped off at a childcare centre at his parents’ gym, leading to their avoiding exercise. He slept in his own crib, rocked to sleep by a parent, but would wake in a panic (alert but distressed) two to three times per month, crying for over an hour until his parents took him into their bed. K also was very particular about where objects were placed in the playroom and would fuss if they were put in the wrong place. He got anxious about deviations in routine (eg, taking a different path on a walk) and had trouble throwing things away (eg, used Band-Aids).
Intervention Feasibility and Outcomes
To demonstrate feasibility, the application of the treatment protocol with both participants is summarised in table 1 . Both participants completed the treatment, in 11 and 10 sessions, respectively. For each, session engagement was rated ‘moderately’ or ‘completely engaged’ at all but one session, and homework adherence was rated as ‘moderate work’ to ‘did everything assigned’ at all but one session.
The quantitative results of the treatment are presented in table 2 . Both children were rated by the clinician as having shown ‘much improvement’ (Clinician Global Impression of Anxiety-Improvement 1 or 2), and both showed changes in quantitative measures of anxiety and family function. In both families, parents rated their satisfaction with the treatment as ‘extremely satisfied’, and felt that they would ‘definitely’ recommend the intervention to a friend. They rated all strategies introduced in the intervention as ‘very-’ or ‘moderately helpful’ and rated the change in their ability to help their child handle anxiety as ‘moderately-’ to ‘very much improved’.
These pilot cases demonstrate the feasibility and acceptability of parent–child CBT for toddlers with anxiety disorders. The two participating families completed the treatment protocol and were consistently engaged with in-session exercises and adherent to between-session skills practice. The cases demonstrate that basic coping skills and exposure practice can be conducted with toddlers.
Although efficacy cannot be determined from uncontrolled case studies, the cases did show promising preliminary results. Both children showed a decrease in number of anxiety disorders, both were rated by the clinician (and parents) as either ‘moderately-’ or ‘much improved’ in their overall anxiety, and both showed increases in their parent-rated ability to cope with their most feared situations. Participant 2 improved on all symptom measures as well. Most significantly, his ITSEA general anxiety, separation distress, inhibition to novelty, negative emotionality, compliance and social relatedness scores and his CBCL total score, internalising score and somatic complaints scale score normalised from clinical to non-clinical range. Participant 1 had a more complicated clinical presentation, and whereas her diagnoses and coping scores improved, her parent-rated symptom scores were more mixed, perhaps related to medical problems which impacted sleep. Beyond changes in the children’s behaviour, family life impairment was reduced for both families, and parental stress was decreased out of clinical range for participant 1. Notably, both children also showed gains in areas of competence, including prosocial peer relations and mastery motivation.
This work extends previous research demonstrating that very young children experience impairing levels of anxiety that are amenable to CBT. Previous studies have found that CBT is as efficacious with older preschool-age children with anxiety disorders as it is with school-aged youth, 14 15 with approximately two-thirds of treated youth demonstrating clinically significant improvement. There is increasing recognition that anxiety disorders start early in childhood, and that there are significant advantages to intervening proximally to their onset, before anxiety symptoms crystallise and impairment accumulates. For example, one study of 1375 consecutive referrals (mean age 10.7) to a paediatric psychopharmacology clinic found that the median age of onset of a child’s first anxiety disorder was 4 years. 30 Children seeking treatment for anxiety often present in middle childhood, for symptoms which began much earlier, exposing the child and family to undue stress for years. By teaching parents and very young children skills to manage anxiety, we hope to give families important tools to navigate the developmental transitions inherent in this age range, and to help children develop a sense of mastery during a critical developmental period. Of course, a larger controlled trial is needed to further evaluate this intervention and its efficacy over time.
Assessing and treating toddlers require a developmentally informed approach. Anxiety and other symptoms may present differently in younger children, and because of limited language and cognitive abstraction capabilities toddlers are not as able to describe their fears and worries. Because some forms of anxiety (eg, separation anxiety, stranger anxiety) are normative, determination of clinically significant levels of anxiety requires an understanding of typical development in toddlerhood and the ability to conduct a detailed assessment with parents and the child using measures normed for this age group (such as the ITSEA and CBCL 1-1/2-5). Similarly, implementing CBT with toddlers and preschoolers requires age-appropriate modifications of empirically supported techniques. The adaptations we used included increased parental involvement in planning exposures, decreased focus on child cognitive restructuring (beyond framing the practice as ‘being brave’ and redirecting the child’s attention to rewarding aspects of the situation), and adaptations to exposure exercises to maximise child participation and motivation (practising at times when the child was rested and not irritable, incorporation of games and reinforcers, and allowing the child maximal choice about when/how to carry out the exposure). The cases we presented demonstrate that existing interventions can be effectively adapted and implemented with children as young as 2 years of age. By sharing the information gleaned from our research, we hope to inform providers who may be less familiar with treating children in this age range and increase their confidence in intervening with very young children.
Dina Hirshfeld-Becker earned her undergraduate degree from Harvard and her doctorate in clinical psychology from Boston University, and completed post-doctoral training at Massachusetts General Hospital. Dr Hirshfeld-Becker is currently co-founder and co-director of the Child Cognitive Behavioral Therapy (CBT) Program in the Department of Psychiatry at MGH and an associate professor of psychology in the Department of Psychiatry at Harvard Medical School. The Child CBT Program offers short-term empirically supported CBT with youths ages 3-24, research in novel treatment adaptations, and clinical training in CBT, including on-line training courses. She pioneered the development and empirical evaluation of one of the first manualized cognitive-behavioral intervention protocols for anxiety in 4- to 7-year-old children, the “Being Brave” program, and has been exploring its use with children with autism spectrum disorder and with younger toddlers and their parents. Dr Hirshfeld-Becker has published numerous articles, reviews, and chapters. Her main research interests include the etiology, development, and treatment of childhood psychiatric disorders, particularly anxiety disorders, and in the study of early risk factors for these disorders.
- Publication history
- Rapid Responses

Hannah, an anxious child Hannah (not a real person) was a 10-year-old girl from a close, supportive family who was described as 'anxious from birth'. She had been a shy, reserved young girl at pre-school, but she integrated well in grade 1 and began making friends and succeeding academically. She complained several times of severe abdominal pain that was worst in the morning and never present at night. She had missed about 20 days of school during the previous year because of the pain. She also avoided school excursions, fearing the bus would crash. She had difficulty falling asleep and frequently asked her parents for their reassurance. Hannah was worried that she and members of her family might die. She was unable to sleep at all before a test. She could not tolerate having her parents on a different floor of the house from herself, and she insisted on securing the house to an unnecessary extent in the evenings, fearing intruders. Her insecurity, need for constant reassurance, and school absenteeism were frustrating and upsetting for her parents. Hannah had no personal history of traumatic events. She exhibits symptoms typical of childhood anxiety disorder, which is thought to occur in about 10% of children, equally in boys and girls before puberty. This type of disorder is diagnosed when anxiety is sufficient to interfere with daily functioning, for example Hannah's school attendance and sleep. These effects can increase and interfere to a progressively greater extent with age-appropriate functioning at home, at school and with peers, and also places sufferers at risk of developing mood disorders or substance abuse disorders in the future. Many children experience fears; fears that are developmentally normal. Children with anxiety disorders, however, experience persistent fears or other symptoms of anxiety for months. Children can experience all the anxiety disorders experienced by adults. However, they can also experience separation anxiety disorder and selective mutism (failure to speak in certain social situations, thought to be related to social anxiety), which are unique to children. The duration of Hannah's difficulties and the symptoms, including inability to sleep, attend school regularly, go on school excursions, or face tests without extreme distress are all developmentally inappropriate, suggesting an anxiety disorder. There is a range of common symptoms seen in anxious children. Symptoms involving thoughts include worrying, requests for reassurance, 'what if.' questions, and upsetting obsessive thoughts. Common symptoms involving behaviours include difficulty in separation, avoiding feared situations, tantrums when faced with fear, 'freezing' or mutism in feared situations, and repetitive rituals, or compulsions. Common symptoms involving feelings include panic attacks, hyperventilation, stomachaches, headaches and insomnia. To screen quickly for one or more anxiety disorders in children, four questions are often useful:
These questions address the main thoughts, behaviours and feelings related to anxiety seen in children. Megan Rodgers wishes to acknowledge an article entitled 'Childhood Anxiety Disorders' written by Dr Manassis, a Staff Psychiatrist at the Hospital for Sick Children and the Center for Addiction and Mental Health in Toronto, Ontario, on which this article is based. Written by Megan Rodgers ADAVIC Volunteer June 2004
Prevalence of social anxiety during COVID-19 pandemic: A systematic review and meta-analysis
Cite this article
The COVID-19 pandemic caused widespread disruption and increased concerns about mental health. One area of particular concern is social anxiety disorder (SAD), as the lockdowns and restrictions have made it difficult for people to engage in social activities. Studies show inconsistency in the prevalence rates reported in different studies, making it difficult to draw a clear picture of the situation. Thus, the study, first attempt to the best of our knowledge, investigates the overall prevalence of SAD during the COVID-19 pandemic. Following PRISMA 2020 guidelines, four academic databases including PubMed, Scopus, Web of Science, and ProQuest, in addition to hand search of reference list of included studies, yielded 338 initial studies, from which 16 were included in the systematic review and meta-analysis. The study found that prevalence of SAD during pandemic was 28% [95% CI: 0.12 to 0.50; I2: 99.6% [based on 16 included studies with 13,961 individuals. After removing seven studies identified as outliers, the pooled prevalence was found to be 34% [95% CI: 0.23 to 0.47; I 2 of 93.1%]. No publication bias was detected. Sub-Group analysis suggested that only the prevalence differed significantly for WHO region sub-group. Additionally, moderator analysis was performed on study-level data, such as age, gender, and risk of bias but no significant changes were found. As the prevalence of SAD was considerable during Covid-19pandemic, mental health support during these challenging times is needed. This is a preview of subscription content, log in via an institution to check access. Access this articleSubscribe and save.
Price includes VAT (Russian Federation) Instant access to the full article PDF. Rent this article via DeepDyve Institutional subscriptions 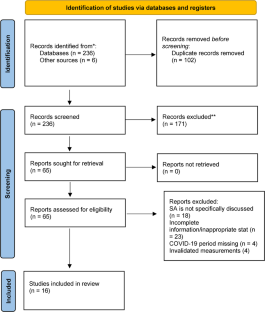 Availability of data and materialGuaranteed. Code availabilityAderka, I. M., McLean, C. P., Huppert, J. D., Davidson, J. R. T., & Foa, E. B. (2013). Fear, avoidance and physiological symptoms during cognitive-behavioral therapy for social anxiety disorder. Behaviour Research and Therapy, 51 (7), 352–358. https://doi.org/10.1016/j.brat.2013.03.007 Article PubMed PubMed Central Google Scholar Agordzo, M. P., Ofosuhene-Mensah, J. K., Krafona, K., & Ekem-Ferguson, G. (2021). Social Anxiety and Self-Compassion in Persons with Alcohol Use Disorders in Ghana. International Journal of Research and Innovation in Social Science, 05 (01), 563–568. https://doi.org/10.47772/IJRISS.2021.5128 Article Google Scholar Alrazeeni, D. (2021). Public anxiety during coronavirus-19 disease (COVID-19) in Saudi Arabia: Indication for a psychological assistance intervention. International Journal of Advanced and Applied Sciences, 8 (4), 12–16. https://doi.org/10.21833/IJAAS.2021.04.002 Alvi, T., Kumar, D., & Tabak, B. A. (2022). Social anxiety and behavioral assessments of social cognition: A systematic review. Journal of Affective Disorders, 311 , 17–30. https://doi.org/10.1016/J.JAD.2022.04.130 Ambusaidi, A., Al-Huseini, S., Alshaqsi, H., AlGhafri, M., Chan, M.-F., Al-Sibani, N., Al-Adawi, S., & Qoronfleh, M. W. (2022). The Prevalence and Sociodemographic Correlates of Social Anxiety Disorder: A Focused National Survey. Chronic Stress, 6 , 247054702210812. https://doi.org/10.1177/24705470221081215 APA. (2013). APA - DSM - Diagnostic and Statistical Manual of Mental Disorders . https://www.appi.org/dsm Google Scholar Armour, C., McGlinchey, E., Butter, S., McAloney-Kocaman, K., & McPherson, K. E. (2021). The COVID-19 Psychological Wellbeing Study: Understanding the Longitudinal Psychosocial Impact of the COVID-19 Pandemic in the UK; a Methodological Overview Paper. Journal of Psychopathology and Behavioral Assessment, 43 (1), 174–190. https://doi.org/10.1007/S10862-020-09841-4 Article PubMed Google Scholar Australian Bureau of Statistics National Study of Mental Health and Wellbeing. (2023). National Study of Mental Health and Wellbeing, 2020–2022| Australian Bureau of Statistics . https://www.abs.gov.au/statistics/health/mental-health/national-study-mental-health-and-wellbeing/latest-release Barnett, M. D., Maciel, I. V., Johnson, D. M., & Ciepluch, I. (2021). Social Anxiety and Perceived Social Support: Gender Differences and the Mediating Role of Communication Styles. Psychological Reports, 124 (1), 70–87. https://doi.org/10.1177/0033294119900975 Biglbauer, S., & Korajlija, A. L. (2020). Social connections, depression and anxiety. Socijalna Psihijatrija, 48 (4), 404–425. https://doi.org/10.24869/SPSIH.2020.404 Bijl, R. V., De Graaf, R., Ravelli, A., Smit, F., & Vollebergh, W. A. M. (2002). Gender and age-specific first incidence of DSM-III-R psychiatric disorders in the general population: Results from the Netherlands Mental Health Survey and Incidence Study (NEMESIS). Social Psychiatry and Psychiatric Epidemiology, 37 (8), 372–379. https://doi.org/10.1007/s00127-002-0566-3 Borenstein, M., Hedges, L. V., Higgins, J. P., & Rothstein, H. R. (2021). Introduction to meta-analysis . John Wiley & Sons. https://books.google.com/books?hl=en&lr=&id=pdQnEAAAQBAJ&oi=fnd&pg=PP1&dq=Introduction+to+Meta-Analysis.+John+Wiley+%26+Sons.&ots=WFUnAUgNR1&sig=WGt_g7G1XuRzNNGTlxav1xcIYOQ Buckner, J. D., Abarno, C. N., Lewis, E. M., Zvolensky, M. J., & Garey, L. (2021). Increases in distress during stay-at-home mandates During the COVID-19 pandemic: A longitudinal study. Psychiatry Research, 298 . https://doi.org/10.1016/J.PSYCHRES.2021.113821 Burkle, F. M., Jr. (2019). Challenges of global public health emergencies: Development of a health-crisis management framework. The Tohoku Journal of Experimental Medicine, 249 (1), 33–41. Campion, J., Javed, A., Sartorius, N., & Marmot, M. (2020). Addressing the public mental health challenge of COVID-19. The Lancet. Psychiatry, 7 (8), 657. Caruana, E. J., Roman, M., Hernández-Sánchez, J., & Solli, P. (2015). Longitudinal Studies. Journal of Thoracic Disease, 7 (11), E537. https://doi.org/10.3978/j.issn.2072-1439.2015.10.63 Cucinotta, D., & Vanelli, M. (2020). WHO Declares COVID-19 a Pandemic. Acta Bio-Medica: Atenei Parmensis, 91 (1), 157–160. https://doi.org/10.23750/abm.v91i1.9397 Davidson, J. R., Hughes, D. L., George, L. K., & Blazer, D. G. (1993). The epidemiology of social phobia: Findings from the Duke Epidemiological Catchment Area Study. Psychological Medicine, 23 (3), 709–718. de Vries Robbé, M., & Willis, G. M. (2017). Assessment of protective factors in clinical practice. Aggression and Violent Behavior, 32 , 55–63. https://doi.org/10.1016/j.avb.2016.12.006 Etikan, I., Musa, S. A., & Alkassim, R. S. (2016). Comparison of convenience sampling and purposive sampling. American Journal of Theoretical and Applied Statistics, 5 (1), 1–4. Fawwaz, A. N., Prihadi, K. D., & Purwaningtyas, E. K. (2022). Studying online from home and social anxiety among university students: The role of societal and interpersonal mattering. International Journal of Evaluation and Research in Education, 11 (3), 1338–1345. https://doi.org/10.11591/IJERE.V11I3.23464 Fehm, L., Pelissolo, A., Furmark, T., & Wittchen, H.-U. (2005). Size and burden of social phobia in Europe. European Neuropsychopharmacology, 15 (4), 453–462. Field, A. P., & Gillett, R. (2010). How to do a meta-analysis. British Journal of Mathematical and Statistical Psychology, 63 (3), 665–694. https://doi.org/10.1348/000711010X502733 Harrer, M., Cuijpers, P., Furukawa, T. A., & Ebert, D. D. (2021). Doing Meta-Analysis with R. Chapman and Hall/CRC . https://doi.org/10.1201/9781003107347 Higgins, J. P., Thompson, S. G., Deeks, J. J., & Altman, D. G. (2003). Measuring Inconsistency in Meta-Analyses. Bmj, 327 (7414), 557–560. PubMed Google Scholar Hofmann, S. G., Anu Asnaani, M. A., & Hinton, D. E. (2010). Cultural aspects in social anxiety and social anxiety disorder. Depression and Anxiety, 27 (12), 1117–1127. https://doi.org/10.1002/da.20759 Huremović, D. (Ed.). (2019). Psychiatry of Pandemics: A Mental Health Response to Infection Outbreak . Springer International Publishing. https://doi.org/10.1007/978-3-030-15346-5 Itani, M. H., Eltannir, E., Tinawi, H., Daher, D., Eltannir, A., & Moukarzel, A. A. (2021). Severe Social Anxiety Among Adolescents During COVID-19 Lockdown. Journal of Patient Experience, 8 , 23743735211038384. https://doi.org/10.1177/23743735211038386 Kaur, A., Ani, A., Sharma, A., & Kumari, V. (2021). Nomophobia and social interaction anxiety among university students. International Journal of Africa Nursing Sciences, 15 . https://doi.org/10.1016/J.IJANS.2021.100352 Kessler, R. C., Petukhova, M., Sampson, N. A., Zaslavsky, A. M., Wittchen, H., Ronald Kessler, C. C., Wiley Online Library, in. (2012). Twelve-month and lifetime prevalence and lifetime morbid risk of anxiety and mood disorders in the United States. International Journal of Methods in Psychiatric Research Int. J. Methods Psychiatr. Res, 21 (3), 169–184. https://doi.org/10.1002/mpr.1359 Kessler, R. C. (2003). The impairments caused by social phobia in the general population: Implications for intervention. Acta Psychiatrica Scandinavica, 108 (s417), 19–27. https://doi.org/10.1034/j.1600-0447.108.s417.2.x Keynejad, R. C., Dua, T., Barbui, C., & Thornicroft, G. (2018). WHO Mental Health Gap Action Programme (mhGAP) Intervention Guide: A systematic review of evidence from low and middle-income countries. BMJ Ment Health, 21 (1), 30–34. Kim, H., Rackoff, G. N., Fitzsimmons-Craft, E. E., Shin, K. E., Zainal, N. H., Schwob, J. T., Eisenberg, D., Wilfley, D. E., Taylor, C. B., & Newman, M. G. (2022). College Mental Health Before and During the COVID-19 Pandemic: Results From a Nationwide Survey. Cognitive Therapy and Research, 46 (1). https://doi.org/10.1007/S10608-021-10241-5 Kok, A. A. L., Pan, K. Y., Rius-Ottenheim, N., Jörg, F., Eikelenboom, M., Horsfall, M., Luteijn, R., van Oppen, P., Rhebergen, D., Schoevers, R. A., Giltay, E. J., & Penninx, B. W. J. H. (2022). Mental health and perceived impact during the first Covid-19 pandemic year: A longitudinal study in Dutch case-control cohorts of persons with and without depressive, anxiety, and obsessive-compulsive disorders. Journal of Affective Disorders, 305 , 85–93. https://doi.org/10.1016/J.JAD.2022.02.056 Krajewska-Kułak, E., Kułak-Bejda, A., Kułak, W., Bejda, G., Łukaszuk, C., Waszkiewicz, N., Cybulski, M., Guzowski, A., Fiłon, J., Aniśko, P., & Popławska, M. (2022). Well-Being at Home During Forced Quarantine Amid the COVID-19 Pandemic. Frontiers in Psychiatry, 13 . https://doi.org/10.3389/FPSYT.2022.846122 Leary, M. R. (1990). Responses to Social Exclusion: Social Anxiety, Jealousy, Loneliness, Depression, and Low Self-Esteem. Journal of Social and Clinical Psychology, 9 (2), 221–229. https://doi.org/10.1521/jscp.1990.9.2.221 Li, D. J., Chou, L. S., Chou, F. H. C., Hsu, S. T., Hsieh, K. Y., Wu, H. C., Kao, W. T., Lin, G. G., Chen, W. J., & Huang, J. J. (2021). COVID-related psychological distress fully mediates the association from social impact to sleep disturbance among patients with chronic schizophrenia. Scientific Reports, 11 (1). https://doi.org/10.1038/S41598-021-96022-2 Liberati, A., Altman, D. G., Tetzlaff, J., Mulrow, C., Gøtzsche, P. C., Ioannidis, J. P. A., Clarke, M., Devereaux, P. J., Kleijnen, J., & Moher, D. (2009). The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ, 339 . https://doi.org/10.1136/BMJ.B2700 Makarova, E. A., Makarova, E. L., & Mishchenko, V. I. (2021). Phenomena of loneliness and fear caused by the mass media threat in the situation of COVID-19 pandemic. International Journal of Media and Information Literacy, 6 (1), 146–155. https://doi.org/10.13187/IJMIL.2021.1.146 McEnery, C., Lim, M. H., Tremain, H., Knowles, A., & Alvarez-Jimenez, M. (2019). Prevalence rate of social anxiety disorder in individuals with a psychotic disorder: A systematic review and meta-analysis. Schizophrenia Research, 208 , 25–33. https://doi.org/10.1016/j.schres.2019.01.045 Miyazaki, Y., Kamatani, M., & Kawahara, J. I. (2021). The influence of social anxiety, trait anxiety, and perceived vulnerability to disease on the frequency of face mask wearing. Shinrigaku Kenkyu, 92 (5), 339–349. https://doi.org/10.4992/JJPSY.92.20063 Moitra, E., Herbert, J. D., & Forman, E. M. (2008). Behavioral avoidance mediates the relationship between anxiety and depressive symptoms among social anxiety disorder patients. Journal of Anxiety Disorders, 22 (7), 1205–1213. https://doi.org/10.1016/j.janxdis.2008.01.002 Nadkarni, A., Hanlon, C., & Patel, V. (2023). Mental Health Care Models in Low-and Middle-Income Countries. In A. Tasman, M. B. Riba, R. D. Alarcón, C. A. Alfonso, S. Kanba, D. M. Ndetei, C. H. Ng, T. G. Schulze, & D. Lecic-Tosevski (Eds.), Tasman’s Psychiatry (pp. 1–47). Springer International Publishing. https://doi.org/10.1007/978-3-030-42825-9_156-1 Chapter Google Scholar Patel, A., Knapp, M., Henderson, J., & Baldwin, D. (2002). The economic consequences of social phobia. Journal of Affective Disorders, 68 (2–3), 221–233. Patel, V., & Prince, M. (2010). Global mental health: A new global health field comes of age. JAMA, 303 (19), 1976–1977. Perugi, G., Simonini, E., Savino, M., Mengali, F., Cassano, G. B., & Akiskal, H. S. (1990). Primary and secondary social phobia: Psychopathologic and familial differentiations. Comprehensive Psychiatry, 31 (3), 245–252. Pragholapati, A. (2020). Covid-19 Impact on Students (pp. 1–6). https://doi.org/10.35542/OSF.IO/895ED Book Google Scholar Quittkat, H. L., Düsing, R., Holtmann, F. J., Buhlmann, U., Svaldi, J., & Vocks, S. (2020). Perceived Impact of Covid-19 Across Different Mental Disorders: A Study on Disorder-Specific Symptoms, Psychosocial Stress and Behavior. Frontiers in Psychology, 11 . https://doi.org/10.3389/fpsyg.2020.586246 Rapee, R. M., Sanderson, W. C., & Barlow, D. H. (1988). Social phobia features across the DSM-III-R anxiety disorders. Journal of Psychopathology and Behavioral Assessment, 10 (3), 287–299. https://doi.org/10.1007/BF00962552 Reinelt, E., Aldinger, M., Stopsack, M., Schwahn, C., John, U., Baumeister, S. E., Grabe, H. J., & Barnow, S. (2014). High social support buffers the effects of 5-HTTLPR genotypes within social anxiety disorder. European Archives of Psychiatry and Clinical Neuroscience, 264 (5), 433–439. https://doi.org/10.1007/s00406-013-0481-5 Ruscio, A. M., Brown, T. A., Chiu, W. T., Sareen, J., Stein, M. B., & Kessler, R. C. (2008). Social fears and social phobia in the USA: Results from the National Comorbidity Survey Replication. Psychological Medicine, 38 (1), 15–28. Salehian, R., Jolfaei, A. G., Naserbakht, M., & Abdi, M. (2021). Posttraumatic stress symptoms and general mental health problems during the covid-19 pandemic in iran: Aweb-based cross-sectional survey. Iranian Journal of Psychiatry and Behavioral Sciences, 15 (3). https://doi.org/10.5812/IJPBS.114432 Shengbo, L., Fiaz, M., Mughal, Y. H., Wisetsri, W., Ullah, I., Ren, D., Kiran, A., & Kumar Kesari, K. (2022). Impact of Dark Triad on Anxiety Disorder: Parallel Mediation Analysis During Pandemic. Frontiers in Psychology, 13 , 914328. https://doi.org/10.3389/fpsyg.2022.914328 Stanbouly, D., & Chuang, S. K. (2021). What are the Psychosocial Consequences of Chronic Mask-Wearing in the COVID-19 Pandemic? Journal of Oral and Maxillofacial Surgery, 79 (9), 1815–1816. https://doi.org/10.1016/J.JOMS.2021.04.014 Suhail, A., Dar, K. A., & Iqbal, N. (2022). COVID-19 related fear and mental health in Indian sample: The buffering effect of support system. Current Psychology, 41 (1), 480–491. https://doi.org/10.1007/S12144-021-01694-8 The ESEMeD, MHEDEA 2000 Investigators. (2004). Prevalence of mental disorders in Europe: Results from the European Study of the Epidemiology of Mental Disorders (ESEMeD) project. Acta Psychiatrica Scandinavica, 109 (s420), 21–27. https://doi.org/10.1111/j.1600-0047.2004.00327.x Torabi, F., Hashemi, M., Zamanian, M., Shayganfard, M., & Yousefichaijan, P. (2023). The Prevalence of Social Anxiety in Children with Chronic Functional Constipation. Journal of Comprehensive Pediatrics, 14 (1). https://doi.org/10.5812/compreped-132384 Tundo, A., Betro’, S., & Necci, R. (2021). What is the impact of covid-19 pandemic on patients with pre-existing mood or anxiety disorder? An observational prospective study. Medicina (Lithuania), 57 (4). https://doi.org/10.3390/MEDICINA57040304 Vriends, N., Becker, E. S., Meyer, A. H., & Margraf, J. (2011). Incidence of DSM-IV social phobia in a community sample of young German women. German Journal of Psychiatry, 14 (2), 80–90. Vriends, N., Bolt, O. C., & Kunz, S. M. (2014). Social anxiety disorder, a lifelong disorder? A review of the spontaneous remission and its predictors. Acta Psychiatrica Scandinavica, 130 (2), 109–122. https://doi.org/10.1111/acps.12249 Wagner, R., Silove, D., Marnane, C., & Rouen, D. (2006). Delays in referral of patients with social phobia, panic disorder and generalized anxiety disorder attending a specialist anxiety clinic. Journal of Anxiety Disorders, 20 (3), 363–371. Wang, C., Pan, R., Wan, X., Tan, Y., Xu, L., Ho, C. S., & Ho, R. C. (2020). Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. International Journal of Environmental Research and Public Health 2020, Vol. 17, Page 1729, 17 (5), 1729. https://doi.org/10.3390/IJERPH17051729 Weiller, E., Bisserbe, J.-C., Boyer, P., Lepine, J.-P., & Lecrubier, Y. (1996). Social phobia in general health care: An unrecognised undertreated disabling disorder. The British Journal of Psychiatry, 168 (2), 169–174. WHO. (2022). Mental disorders . Https://Www.Who.Int/News-Room/Fact-Sheets/Detail/Mental-Disorders. WHO World Mental Health Survey Collaborators, Stein, D. J., Lim, C. C. W., Roest, A. M., De Jonge, P., Aguilar-Gaxiola, S., Al-Hamzawi, A., Alonso, J., Benjet, C., Bromet, E. J., Bruffaerts, R., De Girolamo, G., Florescu, S., Gureje, O., Haro, J. M., Harris, M. G., He, Y., Hinkov, H., Horiguchi, I., & Scott, K. M. (2017). The cross-national epidemiology of social anxiety disorder: Data from the World Mental Health Survey Initiative. BMC Medicine, 15 (1), 143. https://doi.org/10.1186/s12916-017-0889-2 Article PubMed Central Google Scholar Yun, P., Xiaohong, H., Zhongping, Y., & Zhujun, Z. (2021). Family Function, Loneliness, Emotion Regulation, and Hope in Secondary Vocational School Students: A Moderated Mediation Model. Frontiers in Public Health, 9 , 722276. https://doi.org/10.3389/fpubh.2021.722276 Zheng, V., & Fung, A. Y. H. (2021). COVID-19, social anxiety, and economic-political crisis in Hong Kong: A public opinion survey’s perspective. The Routledge Handbook of Public Health and the Community , 150–170. https://doi.org/10.4324/9781003119111-15 Download references Author informationAuthors and affiliations. Department of Psychology, Jamia Millia Islamia, New Delhi, India Mohammad Hashim, Meena Osmany & Naved Iqbal Social Determinants of Health Research Center, Research Institute for Prevention of Non-Communicable Diseases, Qazvin University of Medical Sciences, Qazvin, Iran Zainab Alimoradi Department of Psychology, Government Degree College Baramulla, Jammu and Kashmir, India Kaiser Ahmad Dar You can also search for this author in PubMed Google Scholar ContributionsMH is the corresponding author and guarantor of the research. He and NI proposed the idea of the research, wrote the first draft, and analysed the result. MO and KAD contributed to data collection and verification. ZA supervised systematic review and meta-analysis portions and suggested appropriate changes. NI supervised the whole process. All 5 members contributed to the critical evaluation of the final manuscript. Corresponding authorCorrespondence to Mohammad Hashim . Ethics declarationsEthics approval, consent to participate, consent for publication, conflicts of interest/competing interests, additional information, publisher’s note. Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations. Supplementary informationSupplementary material 1, rights and permissions. Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law. Reprints and permissions About this articleHashim, M., Osmany, M., Alimoradi, Z. et al. Prevalence of social anxiety during COVID-19 pandemic: A systematic review and meta-analysis. Curr Psychol (2024). https://doi.org/10.1007/s12144-024-06617-x Download citation Accepted : 23 August 2024 Published : 29 August 2024 DOI : https://doi.org/10.1007/s12144-024-06617-x Share this articleAnyone you share the following link with will be able to read this content: Sorry, a shareable link is not currently available for this article. Provided by the Springer Nature SharedIt content-sharing initiative
Thank you for visiting nature.com. You are using a browser version with limited support for CSS. To obtain the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in Internet Explorer). In the meantime, to ensure continued support, we are displaying the site without styles and JavaScript.
The impact of COVID-19 on livelihood assets: a case study of high-value crop farmers in North-West Bangladesh
Scientific Reports volume 14 , Article number: 20121 ( 2024 ) Cite this article Metrics details
The COVID-19 pandemic has had a catastrophic impact on public health, extending to the food system and people's livelihoods worldwide, including Bangladesh. This study aimed to ascertain the COVID-19 pandemic impacts on livelihood assets in the North-Western areas (Rajshahi and Rangpur) of Bangladesh. Primary data were collected from 320 farmers engaged in high-value agriculture using a multistage sampling method. The data were analysed using first-order structural equation modelling. The findings reveal a significant impact (p < 0.01) of the pandemic on all livelihood assets in Bangladesh. Notably, human assets exhibited the highest impact, with a coefficient of 0.740, followed sequentially by financial (0.709), social (0.684), natural (0.600), physical (0.542), and psychological (0.537) assets. Government-imposed lockdowns and mobility restrictions were identified as the major causes of the pandemic's negative effects on livelihoods, which included lost income, rising food prices, decreased purchasing power, inadequate access to food and medical supplies, increased social insecurity, and a rise in depression, worry, and anxiety among farmers. The effects of COVID-19 and associated policy measures on the livelihoods of high-value crop farmers have reversed substantial economic and nutritional advances gained over the previous decade. This study suggests attention to the sustainable livelihoods of farmers through direct cash transfer and input incentive programs to minimize their vulnerability to a pandemic like COVID-19 or any other crisis in the future. IntroductionThe SARS-CoV-2 virus, which causes COVID-19, emerged as a threat to public health around the world, and on March 11, 2020, it was declared a worldwide pandemic by the World Health Organization 1 . In Bangladesh, the disease was first detected on March 7, 2020 2 . Bangladesh experienced its 1st phase of lockdown in March–May 2020, drastically disrupted food value chains by restricting the movement of people and commodities. This distribution led to growing rates of food loss and waste, supply chain disruption, and declining product demand 2 . Globally, food insecurity rose due to the disruption of supply chains, resulting in prices and production costs 3 . The COVID-19 pandemic presents an opportunity to study a severe shock to food systems and underscores the importance of access to livelihood assets in buffering against such shocks. Livelihood assets refer to the resources and capabilities that individuals and communities possess, influencing their ability to cope with stresses and shocks and to recover and maintain their livelihoods sustainably 4 , 5 . People in developing nations rely on a variety of resources, including capital and assets, to support their daily lives. Five subsistence assets—natural, physical, financial, human, and social—are used to classify livelihood assets 6 . Psychological factors were added based on the COVID-19 pandemic situation. These assets play an important role in the survival of sustainable rural and urban livelihoods 7 . Not all shocks are anticipated to have the same impact on assets and outcomes related to livelihoods, but shocks such as the pandemic can undermine some or all assets and have a detrimental impact on livelihoods 8 . The COVID-19 has profoundly affected various aspects of life globally. Previous outbreaks, such as Middle East respiratory syndrome (MERS), severe acute respiratory syndrome (SARS), and Ebola, have been extensively studied and have shown to significantly disrupt agricultural labor and output 9 , 10 , 11 . The substantial impacts of COVID-19 on agriculture underscore the importance of a sustainable livelihood strategy that considers different capital assets—natural, economic, financial, human, and social 12 , 13 , 14 , 15 , 16 , 17 . The multidimensional effects of the epidemic on employment, food availability, and market dynamics have resulted in significant food insecurity for daily wage workers 18 , 19 , 20 . Due to COVID-19, there have been substantial disruptions in agricultural productivity and food value chains, as identified in prior research. Due to labor shortages, transportation restrictions, and difficulties in obtaining agricultural inputs have led to increased production costs 21 , 22 . Farmers also encountered challenges in harvesting crops and transporting products to the market, resulted in higher food transportation costs 23 . Labor shortages, further impeded productivity and market access was restricted for sellers and purchasers due to travel restrictions 24 , 25 , 26 , 27 . Furthermore, financial challenges faced by farmers were exacerbated by a decrease in consumer demand for perishables, price increases, and reduced earnings among informal laborers 28 , 29 . This study focuses on farmers engaged in the production of high-value agriculture, such as vegetables. In general, agricultural products that are eaten either fresh or processed and have a substantially higher value (per weight or unit) in the market are considered high-value agriculture 30 . In developing countries like Bangladesh, high-value agricultural practices are important to achieve the sustainable development goals (SDG), particularly SDG 2.3, which describes 2030 as a doubling of the agricultural productivity and incomes of small-scale food producers 31 . Previous studies have examined the impact of COVID-19 on rural livelihood, food safety, dietary diversity, and food security 18 , 32 , 33 , 34 , 35 , 36 , 37 . However, no systematic study has been found concerning how the pandemic impacted the livelihood assets of farmers engaged in high-value agriculture. The study was conducted in four districts of the North-Western (NW) region of Bangladesh, a region with considerable agricultural significance and vulnerability to natural and socioeconomic challenges. The decision to focus on this region was based on its diverse livelihoods, potential for policy impact, and the need to address existing research gaps. Farmers in this region continuously fight against natural disasters, illiteracy, and other development problems 38 . This study offers several novel aspects. Unlike past research focusing on individual aspects of livelihood and farming systems individually, particularly either economic well-being or social aspects 32 , 36 , 37 , 39 , 40 , this study examines the impact of COVID-19 on six dimensions of livelihood assets (financial, social, human, natural, physical, and psychological factors) combined, providing more robust findings. Additionally, this study specifically focuses on high-value crops, which are crucial for commercial farming, whereas other studies broadly focus on farming systems. Conducted in 2022, the study generates more robust, longer-term findings compared to studies conducted immediately after the outbreak of COVID-19 in 2020 2 , 18 , 19 , 32 , 33 , 34 , 35 , 36 , 39 , 40 , 41 , 42 . Finally, the use of Structural Equation Modeling (SEM) is employed in this study for research hypotheses testing since it is more robust than other studies using the OLS model or qualitative approaches 43 . The key methodological strength of this study is the application of first-order SEM to evaluate the impact of COVID-19 on livelihood assets. SEM enables the analysis of complex relationships between observed and latent variables, facilitating a more nuanced comprehension of the interrelations and impacts of various dimensions of livelihood assets during the pandemic. As the global food systems have been significantly disrupted by the COVID-19 pandemic, which has resulted in intensified food insecurity, it is essential to comprehend the effects to develop strategies that will improve the sustainability and resilience of agricultural systems and livelihoods, particularly in developing countries such as Bangladesh. The study offers a comprehensive evaluation of the pandemic's effects on six dimensions of livelihood assets among high-value crop farmers, providing critical insights for policymakers to develop evidence-based recommendations for targeted interventions. This research provides critical insights into the multifaceted impacts of the COVID-19 pandemic on high-value crop producers in Bangladesh, thereby facilitating the creation of more sustainable and resilient food systems. The findings are especially pertinent for policymakers, as they offer evidence-based recommendations for targeted interventions that can improve the resilience of rural communities and ensure food security. This study contributes valuable knowledge to the existing body of research by addressing a research gap on the pandemic's impact on high-value crop producers. The paper is divided into six sections. The literature review is presented in Section " Literature review ", followed by the methodology in Section " Methodology ". Section " Results " presents the results, whereas Section " Discussion " presents the discussion. Conclusions and policy recommendations are presented in the final section. Literature reviewIn Bangladesh, approximately 16.2 million farm households, predominantly smallholders (with 0.05–2.49 acres of land), engage in commercial vegetable production, utilizing approximately 2.63% of the total cultivable land 44 . While the immediate consequences of COVID-19 were widely felt 21 , on-farm challenges also emerged. Assessment of agricultural inputs became more difficult, leading to increased production costs alongside labor shortages and transportation hurdles. Farmers experienced obstacles in harvesting crops or transporting goods to markets due to mobility restrictions 22 . The reduced number of vehicles on the road contributed to heightened food transportation costs 23 . Labor shortages further hampered agricultural productivity, while travel restrictions constrained access to markets for both sellers and buyers 24 . Although there was a surplus of physical labor due to the return of migrant workers from other countries and unemployed urban workers to rural areas, restrictions on the movement of migrant workers resulted in labor shortage 25 , 26 , 27 . In addition to production issues, farmers encountered market challenges stemming from a decrease in consumer demand for goods, especially perishables. High-value agricultural products such as fruits and vegetables, meat, fish, milk, and eggs, which typically have strong income elasticities, experienced substantial declines in demand due to reduced earnings among non-salaried informal workers and price hikes, particularly in metropolitan areas 28 . As consumer demand dwindled, supply disruptions persisted, forcing farmers to sell below cost and leading to significant financial hardships 29 . These production disruptions are not unique to the COVID-19 pandemic but have been observed in both emerging and industrialized nations during previous epidemics. Diseases like Ebola, MERS, and SARS primarily disrupted food systems in the regions where they occurred 9 . By affecting agricultural labor forces and hindering other input factors 10 , these diseases significantly reduced agricultural production 11 . Similarly, COVID-19 has had a profound impact on the agricultural production industry, which serves as the cornerstone of the food system. The sustainable livelihoods approach offers a framework for understanding the purpose, significance, and dimensions of human development 12 . It encompasses various forms of capital, including natural, economic, financial, human, and social, all of which contribute to sustainable livelihoods. Natural capital refers to the ownership or shared management of natural resources such as climate, soil fertility, and water sources, which are essential for production 13 . Human capital encompasses all human potential that enables individuals to pursue various livelihood activities and achieve communal objectives 14 . Physical capital comprises infrastructure and means of production necessary to support livelihoods 15 . Social capital emerges from social organizations and encompasses characteristics like trust, norms, and collaboration, which can strengthen society by promoting coordination and cooperation for various benefits 16 . Financial assets indicate access to different resources, particularly savings and loans 17 . Both direct loans and savings serve as forms of productive capital that can be converted into other types of capital or utilized for immediate consumption. COVID-19 had a profound impact on rural livelihoods, manifesting in several ways 19 , 20 . For example, many individuals lost their jobs due to regulations on social interactions, self-imposed isolation, and travel restrictions. Additionally, panic buying resulted in unpredictable food supplies. The significant disruptions to the agriculture industry led to severe food shortages, lower wages and significant food insecurity among Bangladesh's daily wage workers, who comprise one-third of the labor force 18 . Labour shortages affected agricultural production, while travel restrictions constrained access to markets for both buyers and sellers 24 . Consequently, prices for agricultural products initially surged in local marketplaces due to a lack of consumers and dealers before subsequently plummeting, particularly for perishable goods like vegetables and fish 42 . Previous research indicates that COVID-19 significantly disrupted households’ ability to access adequate food, with 82.5% of respondents expressing concerns about food security, rising costs, and disruptions in local markets 36 . The pandemic also had adverse effects on agricultural production, sales, prices, and income, with over 80% of farms experiencing sales declines and 20% faced severe losses, while 90% reported price reductions 39 . The vulnerability of households to the COVID-19 outbreak encompasses social, economic, human, physical, and psychological dimensions, which significantly impact their resilience 40 . The diverse impacts of shocks on rural households highlight the disparities in their capital assets and subsistence strategies, influencing their ability to recover from market or natural shocks 45 . For rural households with limited access to natural resources, procuring food and accumulating other assets becomes challenging, exacerbating vulnerabilities 46 . Furthermore, the trauma experienced during crises can lead people to rely more heavily on their social networks for support 47 . Shocks such as epidemics can severely impact various livelihood assets (financial, social, human, physical, and natural assets), as evidenced by the negative effects of Ebola on home crop production in Liberia, exacerbating food insecurity 48 . While previous studies have addressed the impacts of epidemics and COVID-19 on individual aspects of livelihoods and farming systems, our research offers a comprehensive perspective by examining the combined vulnerability of six dimensions of livelihood assets (financial, social, human, physical, natural, and psychological assets). By including psychological assets our study acknowledges the holistic nature of livelihood vulnerability, recognizing that mental well-being influences and interacts with traditional livelihood assets. This comprehensive approach enables a more accurate assessment of the multifaceted impacts of COVID-19 on people's lives and livelihoods. MethodologyThe selection of the NW region of Bangladesh for this study was deliberate, considering its significant cultivation of high-value crops and prevalent poverty conditions, particularly exacerbated during the COVID-19 pandemic. Rural livelihoods in these regions rely heavily on high-value agriculture, making them vital study areas. Additionally, the NW region is susceptible to natural disasters, further complicating the socio-economic landscape. The pandemic exacerbated existing vulnerabilities, pushing households deeper into poverty 49 . The study focused on four districts within the NW region: Dinajpur, Rangpur, Bogura, and Pabna (see Fig. 1 ) chosen in collaboration with the Department of Agricultural Extension (DAE).  Study area. The authors used ArcGIS 10.8 ( https://www.arcgis.com/index.html ) to produce the map, employing the administrative shapefile of Bangladesh in the process. Shapefile republished from the Bangladesh Agricultural Research Council (BARC) database ( http://maps.barcapps.gov.bd/index.php ) under a CC BY license, with permission from Computer and GIS unit, BARC, original copyright 2014. The mWater surveyor app was used to conduct direct interviews using a structured questionnaire for the collection of primary data. A total of 320 farmers, 80 from each district, were surveyed from eight upazilas in four districts of the North-West region, employing a multistage sampling technique (Table 1 ). Initially, the selection of the four districts in our study was based on their prominence in high-value crop farming within the North-West region. In this study, two Upazilas were purposively selected from each district to capture the geographic and socioeconomic diversity within the districts, ensuring a comprehensive representation of different agricultural practices and livelihood conditions. Subsequently, farmers were randomly selected by drawing numbers from a compiled list of high-value vegetable growers, provided by the Sub-Assistant Agricultural Officer of the DAE from the respective agricultural blocks. An equal sample size of 40 participants per Upazila was adopted to ensure statistical consistency and enable reliable comparative analysis across Upazilas, thereby enhancing the robustness of our findings. The total sample size was determined using the following formula 50 . where p is the predicted proportion of respondents and n is the sample size, the p-value of 0.50 was utilized to obtain the greatest number of respondents. The acceptable margin of error is represented by e, which is equal to 0.06, and Z stands for standard error for a 95% confidence level. So, the sample size would be, Although the estimator suggested a sample size of 266, we selected to survey 320 farming households from four districts in Bangladesh to reduce the margin of error by an additional 20%. Farmers from the study area were selected using simple random sampling. These individuals, known as high-value agricultural producers, specialize in cultivating crops such as brinjal, pointed gourd, beans, cabbage, cauliflower, tomato, carrot, and bottle gourd. The survey was conducted between May and June 2022, relying on respondents’ memories for data for 2019 and 2022. This sample had been used previously somewhere else. A structured questionnaire was designed (as detailed in Supplementary file 2 ), covering demographic characteristics, livelihood assets, and psychological factors of high-value crop farming. Equal weight was given to each of the six livelihood diversification options when selecting responses. The questionnaire underwent pre-testing by the authors before being finalized. The study did not use the pre-tested data in the analysis. Data collection was conducted via face-to-face interviews using the finalised questionnaire, which was exported to the mWater portal, a web-based digital data collection tool. In this study, we examine the impact of COVID-19 on the assets of high-value crop farmers in Bangladesh's NW region using a reflecting model. Reflective models are applicable when indicators represent underlying latent constructs, meaning changes in the latent variable are mirrored in changes in the indicators 51 . The financial, social, physical, human, natural, and psychological resources examined in this study are considered reflective, as they are expected to adapt to changes in the underlying latent concept of livelihood impact. The collected primary data were used to assess the impact of COVID-19 on livelihood assets. First-order partial least square structural equation modelling (PLS-SEM) was applied to determine these impacts using SmartPLS 4 software 52 . Structural equation modelling is a hypothesis testing method that evaluates whether the indicators accurately measure latent variables. As latent variables cannot be directly measured, they are inferred from the observable. Due to its flexibility in modelling complex interactions without making rigid assumptions about data distribution, PLS-SEM is well suited for this purpose. It is particularly useful for analyzing data from small samples providing valid findings 43 . Figure 2 presents the conceptual model linking the relationship between six livelihood factors and COVID-19 impacts. Twenty-seven statements were constructed to define six livelihood assets (see Appendix Table 1 ). The scales and attributes were derived from previous research 5 , and these were tailored to the context of vulnerable livelihood assets in Bangladesh. Farmers responses to these statements were collected using a five-point Likert scale (1 = very low to 5 = very high). COVID-19 was treated as a dependent variable, categorised as 0 = before COVID-19 and 1 = during COVID-19. The study identified five categories of assets: natural, physical, financial, human, and social 6 . These assets play a vital role in survival strategies for rural and urban livelihoods 7 . Additionally, psychological assets, such as fear of infection, social tensions, and depression, were considered due to the pandemic's profound effect on mental health and well-being. The capacity of farmers to manage tension and anxiety became an integral component of their overall vulnerability. Psychological vulnerability (defined as PhAV) was added based on the COVID-19 pandemic when anxiety, worry, and depression were high among the farmers 53 . Financial assets were chosen as indicators to capture the pandemic's economic effects. Farmers were expected to experience income loss, increased food prices diminished purchasing power, and unemployment as a result of the pandemic. Financial asset vulnerabilities (FAV) indicate income loss, decreased purchasing power, increased food prices, unemployment, poverty, and inequality. Social resources that people utilize to support their livelihoods are referred to as social property because they are part of a network of social ties between individuals or groups 54 . Farmers frequently communicate face-to-face with friends and family members to demonstrate their skills and knowledge of agricultural operations 55 . Social assets were chosen as indicators due to their involvement in crisis resilience 56 . It was anticipated that the pandemic's impact on social interactions, trust in information sources, and social insecurity would hinder farmers' ability to respond to the crisis' challenges. Social asset vulnerability (SAV) encompasses trust among individuals, social solidarity, trust in media information, changes in traditions and customs, and social insecurity. Given the threat posed by the pandemic to public health, assessing the vulnerability of human assets becomes crucial. Anticipated outcomes of the pandemic, such as the closure of educational institutions, limited access to medical services, and psychological distress, could significantly impact high-value crop producers. Human assets vulnerability (HAV) is therefore characterised by factors such as the closure of educational institutions, inadequate access to medical staff, and insufficient health information and counselling services. Physical assets typically encompass essential amenities and infrastructure supporting agricultural production and livelihoods such as tractors, water supply canals, and roads. Disruptions in the supply chain caused by the COVID-19 pandemic have limited access to vital agricultural inputs and equipment. Understanding the pandemic’s impact on agricultural productivity necessitates a thorough evaluation of physical assets vulnerability. (PAV), which includes factors like inadequate access to pharmaceutical items, limited availability of disinfectants and detergents, and a shortage of reliable resources providing information about COVID-19 treatment. Natural assets refer to the natural properties relied upon for survival and progress. Disruptions to farming operations, brought about by the pandemic, are of utmost importance, as they can significantly affect farmers' ability to sustain themselves. Natural assets vulnerability (NAV) encompasses delays in agricultural activities, underutilization of natural and recreational resources, decreased agricultural outputs, and farmers’ hesitancy to plan crop production 55 , 57 . Detailed descriptions of these assets are provided in Appendix Table 1 .  A conceptual model. To estimate the impacts of COVID-19 on different livelihood assets, we constructed and estimated the following six equations (Eqs. 1 – 6 ), These conceptual equations illustrate our aim to estimate the impacts of COVID-19 on various livelihood assets. The following six hypotheses were formulated to support the above six equations: H 1 = The COVID-19 has a substantial impact on the vulnerability of financial assets. H 2 = The COVID-19 has a substantial impact on the vulnerability of social assets. H 3 = The COVID-19 has a substantial impact on the vulnerability of human assets. H 4 = The COVID-19 has a substantial impact on the vulnerability of physical assets. H 5 = The COVID-19 has a substantial impact on the vulnerability of natural assets. H 6 = The COVID-19 has a substantial impact on the vulnerability of psychological assets. As a result, three steps were taken to ensure the precision of the measurement model: (1) Model dependability and validity, (2) Uni-dimensionality, and (3) Diagnostic analysis, all of which were applied to the effect of COVID-19 on means of subsistence. In assessing reliability, indicators are evaluated based on their consistency in measuring a particular component. When the construct explains more than 50% of the variation of the indicator, as is the case when loading is above 0.60, the indicator is said to have a satisfactory level of dependability 58 . When evaluating reliability, a higher score is better. Reliability levels that are “acceptable to good” are explained by results between 0.70 and 0.95. Next, the average extracted variance was used to determine the convergent validity (AVE). The AVE must be 0.50 or greater to be considered valid, meaning that the construct must account for (at least) 50% of the variance of its elements. Assessing the discriminant validity is the final stage. Finally, discriminant validity is assessed using Fornell–Larcker's criterion, which examines correlations between constructs. The suggested threshold is a value of the Fornell–Larcker criterion of 0.90. Ethical approvalThis study received approval from the Research Ethics Committee of Bangladesh Agricultural University, Mymensingh, Bangladesh (BAU-REC-2022-102) on April 20, 2022. The study was performed in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants and the questionnaires were anonymized to protect their privacy. Participants were also given the option to decline participation in the survey if they chose to do so. Socio-demographic characteristics of the respondentsFarmers' socio-demographic characteristics are explained in Table 2 . The average age of the respondents during COVID-19 was 44.26 years. The mean household size was around five members. About 80% of farmers had various levels of literacy, ranging from primary to upper education. The results also demonstrate a decrease in the average total income of agricultural households during the pandemic. Specifically, the average income from vegetable cultivation decreased by 6,477 Taka, leading to reductions in expenditure. To cope with the income loss, farmers reduced their meals, resulting in an average reduction of 2,197 Taka in monthly household expenditure. Each latent variable was operationalized through several indicators (as detailed in Appendix Table 1 ). Financial and social assets were represented by five indicators each; while natural assets had three indicators. Physical, human assets and psychological factors were represented by four indicators. The relationships between the latent variables and their respective indicators are presented in Table 3 . The findings revealed that the scores assigned to all assessed indicators of financial asset vulnerability ranged above three, indicating high to very high response. The pandemic had a significant income and purchasing power, leading to increased food prices, and reduced employment opportunities, and decreased incomes. Consequently, farmers had to reduce their expenditures by rationing basic needs such as food. The analysis also revealed a notable level of financial stress, as individuals had to ration food to accommodate other necessities. An inverse relationship was found to exist between farmers’ investments in social assets and vulnerability. Some highlighted outcomes included social distrust, particularly within communities and towards national information resources, erosion of social cohesion and solidarity, as well as heightened social vulnerability. Many of these changes were attributed to social distancing measures and restrictions on gatherings, which hindered relationships that typically offer social support. Overall, human assets remained more vulnerable in specific areas, including education and health sectors. School closings disrupted children’s education and hindered the long-term development of human capital. Additionally, inadequate access to medical services and health information complicated households' ability to manage their health during the pandemic. Health concerns and mobility limitations also reduced labour availability, leading to lower agricultural output. Farmers faced significant challenges in obtaining essential goods and/or services such as disinfectants, sanitary products, and medications. Delays in planting and harvesting were common due to labour shortages and movement restrictions. Market access was also restricted, affected the physical transportation of goods, which further strained physical resources. Another example of the vulnerability of natural assets was seen in the postponement of the farming seasons, resulting in reduced production and efficiency. Farmers hesitated to invest in the next planting season due to uncertainty. Input constraints and limited extension services, crucial for managing natural resources, resulted in inefficient use of the resources. The study also demonstrated that farmers experienced adverse effects on their psychological health due to the COVID-19 outbreak. The uncertainty and health risks posed by the epidemic increased the prevalence of depression and anxiety. Farmers grappled with the social and economic consequences, which led to heightened social tensions and frustrations. Coping strategies, including reduced food intake and increased reliance on social support networks, were employed to deal with the stress of revenue loss and changed behaviours. Confirmatory factor analysis (CFA)The structure of factors was assessed using CFA, which relied on factor loadings to test the validity of the factors. The threshold values for combined reliability, Cronbach’s α coefficient, and average extracted variance for each structure in the intended model were greater than 0.60, 0.70, and 0.50, respectively. The reliability and validity of all the latent variables are shown in Table 4 . We found that the factor loading values of SAV3 and HAV1 were less than 0.70. Given that the factor loadings did not exceed the cut-off, this suggests that these two factors were invalid. Besides, the coefficient of determination (CR) and Cronbach α were used to determine the latent constructs’ reliability. Thus, the measurement model findings show that for all the latent variables, the least value of Cronbach's alpha and CR was larger than 0.70. Furthermore, all AVE values were above 0.50, indicating convergent validity. After excluding the two invalid factors (SAV3 and HAV1), the convergent validity and reliability were re-estimated. Since all the factor loadings exceeded the cut-off, we concluded that none of the factors were invalid (Table 4 ). Therefore, the results of the measurement model indicate that all the minimum values of Cronbach’s α and CR were greater than 0.70, suggesting that all the constructs were statistically reliable. The relationship between the variables is instead determined using convergent validity 59 . Convergent validity was assessed using the same study, which gave the AVE threshold of 0.50. As the lowest validity was determined to be 0.561, which exceeded 0.50, the results suggest that all the latent constructs have acceptable convergent validity. The predictive value of the model was assessed using the R-square value. The R-square values indicate that the variance in COVID-19 explained 49.6%, 46.6%, 54.2%, 29.3%, 35.8%, and 28.6% in financial, social, human, physical, natural, and psychological assets vulnerability, respectively. Assessment of discriminant validityThe Fornell–Larcker criterion was applied to evaluate discriminant validity by establishing the degree to which one latent concept is distinguishable from the other. The study claimed that 0.90 is the highest figure appropriate in this case. Consequently, none of the connections had a value greater than 0.90 (Table 5 ), showing that no violation of the discriminant validity assumption occurred. Path coefficient assessmentThe study utilised bootstrapping (5,000 iterations), a resampling approach, to assess the importance of each component in explaining the others. The path coefficient results are presented in Table 6 . We find that the impact of COVID-19 on all livelihood assets was statistically significant at 1% (Table 6 ). Figure 1 in the appendix presents the outcomes of the path model. All latent variables were significantly affected by COVID-19 (financial assets, social assets, human assets, physical assets, natural assets, and psychological factors). The p-values and standardized regression coefficients are presented in the numbers on the path relationships. The p-values were less than 0.01 for all latent variables, indicating significance at the 1% level. On the other hand, the values from latent variables to indicators imply the relationship between indicators and latent variables. For all the indicators, the p-values were less than 0.01, indicating significance at the 1% level. This suggests that all the indicators were related to the latent variables. We discovered that COVID-19 had the greatest effect on financial assets (coefficient = 0.709; p-value < 0.01). The positive effect indicates that income and purchasing power were reduced by the COVID-19 pandemic due to inflated food prices, decreased employment opportunities, and increased costs of rural households. Additionally, COVID-19 had a statistically significant and positive effect on social assets (coefficient = 0.684, p-value < 0.01), indicating that due to the COVID-19 pandemic, people's trust in each other declined, social solidarity diminished, and the level of social insecurity increased. The lowest impact of COVID-19 was on human assets (coefficient = 0.740, p-value < 0.01), which implies the COVID-19 pandemic forced educational institutions to close, there was a lack of adequate health information and a lack of adequate medical staff. COVID-19 affected physical assets significantly and positively (coefficient = 0.542, p-value < 0.01), showing that the COVID-19 pandemic reduced sufficient access to pharmaceutical items, disinfectants, sanitary detergents, and reliable medical information. Furthermore, COVID-19 had a statistically significant and favourable influence on natural assets (coefficient = 0.600, p-value < 0.01), indicating that due to the COVID-19 pandemic, farming activities (fertilization, harvesting etc.) were delayed, agricultural output decreased, and farmers were reluctant to plan to grow their crops. COVID-19 also had a significant and positive impact on psychological factors (coefficient = 0.537, p-value < 0.01), indicating that due to the COVID-19 pandemic, farmers were worried about getting COVID-19, social tensions were high, and depression and disappointment increased. The impact of COVID-19 was less on physical assets and psychological assets compared to other assets. The impact of COVID-19 on assets used for sustaining livelihoods has been thoroughly examined. According to the path analysis, COVID-19 had a substantial influence on all categories, including financial, social, physical, human, natural, and psychological assets. This is consistent with most earlier studies, which have also observed a strong influence of COVID-19 on rural livelihoods 5 . Figure 3 illustrates the significant impact of COVID-19 on the assets supporting the livelihoods of farmers engaged in high-value agriculture in the NW regions of Bangladesh.  TreeMap illustrates the consequences of COVID-19 on six livelihood domains. Note: The number in the figure shows the percentage of farmers who ‘agreed’ to ‘strongly agreed’ with the statement. The COVID-19 pandemic has been found to have a statistically significant and considerable effect on the vulnerability of financial assets within the high-value crop farming sector. According to our findings, 91.3% of farmers believed that the COVID-19 pandemic had decreased income and purchasing power in rural households. Similar results were reported by Kundu et al. 34 . Additionally, around 78% of farmers concurred that the pandemic had led to an increase in food prices 60 . This rise in food costs forced many farmers to go without eating, contributing to widespread malnutrition. Moreover, approximately, 77.5% of farmers stated that rural household employment had decreased due to the pandemic, a trend confirmed by Mandal et al. 61 . Many rural residents feared that poverty and inequality would worsen if the pandemic persisted, with 86.3% of farmers holding this view 62 . Additionally, about 71% of farmers believed that the COVID-19 epidemic was responsible for rising living expenses 63 . These findings highlight the tangible negative impact of the pandemic on the economic dimensions of the farmers’ livelihoods. Farmers faced a decline in income, a reduction in their ability to purchase goods and services, and an increased susceptibility to financial risks, attributed to factors such as escalation of food prices and disruptions in the economy. School dropout became a significant challenge in Bangladesh during the COVID-19 pandemic due to various factors, including limited internet access in rural areas, a lack of electronic devices, high costs of internet, early marriage and maternal age, prolonged closures of educational institutions, and inadequate teacher preparation for online learning 64 . Over 95% of farmers agreed that the pandemic had contributed to increased school dropout rates due to limited access to educational facilities 65 . Additionally, 70.6% of farmers agreed that the scarcity of medical personnel and lack of healthcare information in rural areas had heightened the risk of COVID-19 infection 66 . These findings suggest that the pandemic had significant implications for both the physical and mental well-being of farmers. The closure of educational institutions, limited access to medical services, and heightened psychological distress underscored the diverse impact on human and psychological resources. The COVID-19 pandemic has significantly affected social assets, with evidence pointing to decreased social solidarity (60%), reduced social trust (59.4%), and increased social insecurity (48.4%), findings that align with those of De Vos 9 . Furthermore, a majority of farmers (80.9%) reported heightened vulnerability to psychological disorders, such as anxiety, stress, and disappointment 67 . These observations highlight the profound impact of the pandemic on the social fabric and mental health of farmers. Challenges in maintaining social bonds, accessing reliable information sources, and managing escalating social tensions and feelings of insecurity have become prevalent. This underscores the societal and psychological consequences of the pandemic on individuals' livelihoods. Approximately 26.6% of farmers acknowledged that various agricultural activities, such as harvesting and fertilizing, were disrupted during the COVID-19 pandemic 68 . Additionally, around 30% of farmers agreed that the rural community struggled to fully comply with quarantine and health standards due to existing facilities and physical layout constraints 69 . As a result, agricultural production declined (23.5% responses), and farmers hesitated to plan future crop cultivation (30.4% responses) 70 . These findings underscore the pandemic’s adverse effects on agricultural productivity, as farmers encountered difficulties accessing essential inputs and infrastructure 37 . This highlights the pressing challenges in safeguarding physical and natural assets amid the crisis. Our results align with previous research highlighting the significant impact of COVID-19 on rural livelihoods. Consistent with Kundu et al. 34 we observed a decrease in income and purchasing power among rural households. Similarly, our findings of rising food prices and resulting malnutrition corroborate those of Rabbi et al. 60 . However, our study identifies distinct causal factors contributing to these impacts. Disruptions of supply chains and reduced labor availability due to mobility restrictions directly affected agricultural productivity and income. Moreover, financial vulnerabilities were compounded by issues with market access, highlighting the interdependent nature of these factors. By focusing on high-value crop farmers, our study provides new insights into specific vulnerabilities within this subgroup, despite the overall consistency with existing research. In a nutshell, the COVID-19 pandemic has had a profound impact on the ability of individuals to maintain their livelihoods, ranging from significant to extreme. The confirmation of all hypotheses underscores the extensive influence of the pandemic on various aspects of high-value crop farmers' livelihoods. Given the heterogeneous nature of these impacts, policymakers must be mindful and develop pro-poor strategies to enhance crisis-resilience capacity, particularly targeting the most vulnerable farm households in Bangladesh. Practical implicationsWhile it is true that the government of Bangladesh has taken proactive measures to address the challenges posed by COVID-19 in the agricultural sector 2 , 71 , it is important to note that the situation remains dynamic. Ongoing research can play a vital role in shaping policy-making in several ways. The broad impact of COVID-19 on farmers’ livelihoods highlights the need for comprehensive, multifaceted policy interventions. By addressing the specific vulnerabilities and underlying causes identified in this study, policymakers can bolster the resilience of rural livelihoods against future crises. Firstly, our current research provides a comprehensive and in-depth analysis of the impact of COVID-19 on livelihood assets, specifically focusing on high-value crop farmers. By quantifying the extent of the pandemic's impact on various assets related to vulnerability, such as human, financial, social, natural, physical, and psychological, our study offers a nuanced understanding of the lingering effects that may not have been fully addressed yet. Secondly, while the government has prioritized the cultivation and export of high-value vegetables 42 , 72 , our research can identify gaps in these policies and shed light on potential vulnerabilities that might still exist within the sector. For instance, our findings highlight the significance of different asset categories, with financial assets being the most impacted. This emphasizes the need for targeted interventions and support mechanisms, such as access to low-interest loans or financial aid, which can further strengthen the resilience of high-value crop farmers. On the other hand, to enhance the accessibility of healthcare and education services in rural areas, policymakers must prioritize investments in digital infrastructure. The healthcare infrastructure must be fortified to mitigate the psychological distress and health risks that producers encounter. Local governance structures and community-based organizations should be instrumental in the development of trust and social cohesion. Furthermore, our research underscores the role of mobility restrictions and lockdowns as factors affecting livelihoods. As these measures could potentially recur in response to various shocks, including new variants or future pandemics, our study offers insights into strategies that can minimize disruptions. Proposing the establishment of a well-structured online marketplace for agricultural products and exploring labor-efficient farming techniques could mitigate the negative consequences of movement restrictions. In summary, while initial policy responses have been implemented, our current research contributes by providing a comprehensive analysis of the multifaceted impact of COVID-19 on high-value crop farmers' livelihoods. By identifying areas of vulnerability and proposing targeted strategies to enhance resilience, our findings can assist policymakers in refining and adapting their approach to ensure the long-term sustainability of this vital sector in the face of evolving challenges. Conclusion, policy recommendations, and limitationsThe study's findings revealed a significant impact of COVID-19 on all categories of assets crucial for sustaining livelihoods. The pandemic and associated governmental restrictions notably affected rural Bangladeshi livelihoods, primarily stemming from lockdowns, mobility limitations, and the repercussions of lost income, rising food prices, and diminished purchasing power. Farm households in a developing country like Bangladesh encounter multifaceted challenges. The unpredictable nature of the COVID-19 situation led to major disruptions in production and marketing activities, income reduction, increase in food prices, and job losses among high-value crop farmers, exacerbating long-term vulnerability. The impact of COVID-19 on financial assets has been profound, creating economic pressure and disrupted the livelihood conditions of farmers. Urgent policy considerations are essential for their recovery. The interdependence of economic, institutional, and social ties within food systems underscores the need for comprehensive interventions. Movement restrictions during the pandemic severely curtailed farmers' access to markets, necessitating the development of a robust online marketplace to mitigate such disruptions, especially considering the perishable nature of agricultural commodities. To address the decrease in both farm and off-farm income and the rise in family expenditure, farmers require easy access to low-interest loans. Government input assistance programs should prioritise agribusiness production, incorporating labor-saving farming techniques and productivity-boosting technologies. Access to food, both physically and financially, is crucial, particularly during public health emergencies. This study underscores the importance of expanding direct cash transfer and food assistance programs and allocating resources to remove barriers to accessing food and other necessities, both in the present and the future. While this study provides insights into the impact of the COVID-19 pandemic on farming households, it is important to acknowledge its limitations. One significant limitation is the reliance on respondents’ memory due to the lack of written documentation regarding income, expenditure, and savings. This reliance on the recall method introduces potential recall bias and may affect the accuracy of the data collected. Additionally, the focus on high-value agricultural practices may limit the generalizability of findings to other social strata within farming communities. Furthermore, the study’s cross-sectional design presents challenges in drawing definitive conclusions about changes in livelihoods over time. Further research could benefit from longitudinal studies to track changes in high-value crop farming livelihood activities more accurately. Moreover, comparative analyses across different socio-economic strata would enhance our understanding of the differential impacts of the pandemic and the effectiveness of various policy interventions and adaptation strategies. This would provide valuable insights for policymakers seeking to mitigate the pandemic's effects on farming communities in developing countries. Data availabilityThe datasets used and/or analysed during the current study available from the corresponding author on reasonable request. Cucinotta, D. & Vanelli, M. WHO declares COVID-19 a pandemic. Acta Biomed. 91 , 157–160 (2020). PubMed PubMed Central Google Scholar Islam, M. T., Talukder, A. K., Siddiqui, M. N. & Islam, T. Tackling the COVID-19 pandemic: The Bangladesh perspective. J. Public Health Res. 9 , 389–397 (2020). Google Scholar Paslakis, G., Dimitropoulos, G. & Katzman, D. K. A call to action to address COVID-19-induced global food insecurity to prevent hunger, malnutrition, and eating pathology. Nutr. Rev. 79 , 114–116 (2021). PubMed Google Scholar Dehghani-Pour, M., Barati, A. A., Azadi, H. & Scheffran, J. Revealing the role of livelihood assets in livelihood strategies: Towards enhancing conservation and livelihood development in the Hara Biosphere Reserve. Iran. Ecol. Indic. 94 , 336–347 (2018). Yazdanpanah, M. et al. The impact of livelihood assets on the food security of farmers in southern Iran during the Covid-19 pandemic. Int. J. Environ. Res. Public Health 18 , 5310 (2021). DFID. Sustainable Livelihoods Guidance Sheets, section 2 .1. Department for International Development (DFID). (1999). Mphande, F. A. Infectious diseases and rural livelihood in developing countries. Infect. Diseas. Rural Livelihood Dev. Count. https://doi.org/10.1007/978-981-10-0428-5 (2016). Article Google Scholar Tsegaye, T. G. et al. Impact of the West African Ebola epidemic on agricultural production and rural welfare evidence from Liberia. PLoS Negl. Trop. Dis. 12 , 1–17 (2018). De Vos, J. The effect of COVID-19 and subsequent social distancing on travel behavior. Transp. Res. Interdiscip. Perspect. 5 , 100121 (2020). Gong, H., Hassink, R., Tan, J. & Huang, D. Regional resilience in times of a pandemic crisis: The case of COVID-19 in China. Tijdschr. voor Econ. en Soc. Geogr. 111 , 497–512 (2020). Lopez, A. D., Mathers, C. D., Ezzati, M., Jamison, D. T. & Murray, C. J. Global and regional burden of disease and risk factors, 2001: Systematic analysis of population health data. Lancet 367 , 1747–1757 (2006). Maas, L. T. The effect of social capital on governance and sustainable livelihood of coastal city community Medan. Procedia Soc. Behav. Sci. 211 , 718–722 (2015). Bhaduri, S., Sinha, K. M. & Knorringa, P. Frugality and cross-sectoral policymaking for food security. NJAS Wageningen J. Life Sci. 84 , 72–79 (2018). DFID. Human Rights for Poor People . (2000). Hussein, K. Livelihoods approaches compared: A multi-agency review of current practice. October 1–61 (2002). Bakarbessy, D. Business independence in social capital review for Asar fish business communities in Laha village, Teluk Ambon district, Ambon city. J. BADATI Ilmu Sos. Hum. 5 , 126–136 (2021). Ellis, F. Rural livelihood diversity in developing countries: Evidence and policy implications (Overseas Dev. Institute, 1999). Mottaleb, K. A., Mainuddin, M. & Sonobe, T. COVID-19 induced economic loss and ensuring food security for vulnerable groups: Policy implications from Bangladesh. PLoS One 15 , e0240709 (2020). CAS PubMed PubMed Central Google Scholar Kar, S. K. et al. COVID-19 pandemic and addiction: Current problems and future concerns. Asian J. Psychiatr. 51 , 102064 (2020). Nicola, M. et al. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 78 , 185–193 (2020). Reardon, T., Bellmare, M. F. & Zilberman, D. How COVID-19 may disrupt food supply chains in developing countries. COVID-19 Glob. Food Secur. 78–80 (2020). Zhang, S. et al. COVID-19 containment: China provides important lessons for global response. Front. Med. 14 , 215–219 (2020). HLPE. Impacts of COVID-19 on food security and nutrition: developing effective policy responses to address the hunger and malnutrition pandemic. HLPE Issues Pap. 1–24 (2021). Zabir, A. A. et al. COVID-19 and food supply in Bangladesh: A review. South Asian J. Soc. Stud. Econ. 10 , 15–23 (2021). Kabir, H., Maple, M. & Usher, K. The impact of COVID-19 on Bangladeshi readymade garment (RMG) workers. J. Public Heal. (United Kingdom) 43 , 47–52 (2021). Karim, M. R., Islam, M. T. & Talukder, B. COVID-19′s impacts on migrant workers from Bangladesh: In search of policy intervention. World Dev. 136 , 105123 (2020). Kumar, P. & Kumar Singh, R. Strategic framework for developing resilience in Agri-Food Supply Chains during COVID 19 pandemic. Int. J. Logist. Res. Appl. 0 , 1–24 (2021). Abhishek, et al. India’s food system in the time of covid-19. Econ. Polit. Wkly. 55 , 12–14 (2020). Meuwissen, M. P. M. et al. Impact of Covid-19 on farming systems in Europe through the lens of resilience thinking. Agric. Syst. 191 , 103152 (2021). Swinnen, J. F. M., Colen, L. & Maertens, M. Constraints to smallholder participation in high-value agriculture in West Africa. in Rebuilding West Africa’s Food Potential (ed. Elbehri, A.) 289–313 (FAO/IFAD, 2013). Pingali, P. & Plavšić, M. Hunger and environmental goals for Asia: Synergies and trade-offs among the SDGs. Environ. Challenges 7 , 100491 (2022). Gatto, M. & Islam, A. H. M. S. Impacts of COVID-19 on rural livelihoods in Bangladesh: Evidence using panel data. PLoS One 16 , e0259264 (2021). Hall, B. Coronavirus and the Implications for Food Systems and Policy. Agrilinks https://agrilinks.org/post/coronavirus-and-implications-food-systems-and-policy (2020). Kundu, S. et al. Determinants of household food security and dietary diversity during the COVID-19 pandemic in Bangladesh. Public Health Nutr. 24 , 1079–1087 (2021). Laborde, D., Martin, W., Swinnen, J. & Vos, R. COVID-19 risks to global food security. Science 369 , 500–502 (2020). ADS CAS PubMed Google Scholar Middendorf, B. J. et al. Smallholder farmer perceptions about the impact of COVID-19 on agriculture and livelihoods in Senegal. Agric. Syst. 190 , 103108 (2021). Dixon, J. M. et al. Response and resilience of Asian agrifood systems to COVID-19: An assessment across twenty-five countries and four regional farming and food systems. Agric. Syst. 193 , 103168 (2021). Mardy, T., Uddin, M. N., Sarker, M. A., Roy, D. & Dunn, E. S. Assessing coping strategies in response to drought: A micro level study in the North-West region of Bangladesh. Climate 6 , 23 (2018). Harris, J., Depenbusch, L., Pal, A. A., Nair, R. M. & Ramasamy, S. Food system disruption: Initial livelihood and dietary effects of COVID-19 on vegetable producers in India. Food Secur. 12 , 841–851 (2020). Pakravan-Charvadeh, M. R. et al. The short-term effects of COVID-19 outbreak on dietary diversity and food security status of Iranian households (A case study in Tehran province). J. Clean. Prod. 281 , 124537 (2021). CAS PubMed Google Scholar Guido, Z., Knudson, C. & Rhiney, K. Will COVID-19 be one shock too many for smallholder coffee livelihoods?. World Dev. 136 , 105172 (2020). Alam, G. M. M. & Khatun, M. N. Impact of COVID-19 on vegetable supply chain and food security: Empirical evidence from Bangladesh. PLoS One 16 , 1–12 (2021). Sharma, P. N. & Kim, K. Model selection in information systems research using partial least squares based structural equation modeling. in International Conference on Interaction Sciences (2012). Weinberger, K. & Genova-II, C. Vegetable production in Bangladesh: Commercialization and rural livelihoods . (2005). Chiwaula, L. & Waibel, H. The role of shocks and risks for the livelihoods of small scale fishing communities of Hadejia-Nguru Wetlands in Nigeria. Proc. Ger. Dev. Econ. Conf. No. 3, (2009). Mbiba, M., Collinson, M., Hunter, L. & Twine, W. Social capital is subordinate to natural capital in buffering rural livelihoods from negative shocks: Insights from rural South Africa. J. Rural Stud. 65 , 12–21 (2019). Berhanu, W. Recurrent Shocks, Poverty Traps and the Degradation of the Social Capital Base of Pastoralism: A Case Study from Southern Ethiopia . CEGA Working Paper Series No. AfD-0916. Center of Evaluation for Global Action. University of California, Berkeley (2009). Gatiso, T. T. et al. The impact of the Ebola virus disease (EVD) epidemic on agricultural production and livelihoods in Liberia. PLoS Negl. Trop. Dis. 12 , e0006580 (2018). Mainuddin, M. et al. Irrigated agriculture in the northwest region of Bangladesh. Canberra, Aust. … (2019). Kothari, C. R. Research methodology : Methods and techniques . (New Age International (P) Limited, 2004). Simonetto, A. Formative and reflective models: State of the art. Electron. J. Appl. Stat. Anal. 5 , 452–457 (2012). MathSciNet Google Scholar Ringle, C. M., Wende, S. & Becker, J.-M. SmartPLS 4. Oststeinbek: SmartPLS. (2022). Thompson, R. et al. Mental health and substance use of farmers in Canada during COVID-19. Int. J. Environ. Res. Public Health 19 , 13566 (2022). Carney, D. et al. Livelihoods appriaches compared: A brief comparison of the livelihoods approaches of the UK Department for International Development (DFID), CARE, Oxfam and the United Nations Development Programme (UNDP) . (1999). Kuang, F., Jin, J., He, R., Ning, J. & Wan, X. Farmers’ livelihood risks, livelihood assets and adaptation strategies in Rugao City, China. J. Environ. Manage. 264 , 110463 (2020). Busic-Sontic, A. & Schubert, R. Social resilience indicators for pandemic crises. Disasters https://doi.org/10.1111/disa.12610 (2023). Article PubMed Google Scholar Baffoe, G. & Matsuda, H. An empirical assessment of rural livelihood assets from gender perspective: Evidence from Ghana. Sustain. Sci. 13 , 815–828 (2018). Brown, T. A. Confirmatory factor analysis for applied research . (A Division of Guilford Publications, Inc. 72 Spring Street, New York, NY 10012, 2015). Wong, K. K. K. Mastering partial least squares structural equation modeling (PLS-SEM) with SmartPLS in 38 hours. Syria Stud. 7 , 37–72 (2015). Rabbi, M. F., Oláh, J., Popp, J., Máté, D. & Kovács, S. Food security and the covid-19 crisis from a consumer buying behaviour perspective—The case of Bangladesh. Foods 10 , 1–20 (2021). Mandal, S. C. et al. The impact of the COVID-19 pandemic on fish consumption and household food security in Dhaka city, Bangladesh. Glob. Food Sec. 29 , 100526 (2021). Patel, J. A. et al. Poverty, inequality and COVID-19: The forgotten vulnerable. Public Health 183 , 110–111 (2020). Diwambuena, J., Musimwa, I. & Tsasa, J.-P. K. Covid-19 and cost of living in developing countries*. Pre print (2020) https://doi.org/10.21203/rs.3.rs-100217/v1 License. Sarker, M. R., Rouf Sarkar, M. A., Alam, M. J., Begum, I. A. & Bhandari, H. Systems thinking on the gendered impacts of COVID-19 in Bangladesh: A systematic review. Heliyon 9 , e13773 (2023). Dutta, S. & Smita, M. K. The Impact of COVID-19 pandemic on tertiary education in Bangladesh: Students’ perspectives. Open J. Soc. Sci. 08 , 53–68 (2020). Ahmed, S. A. K. S. et al. Impact of the societal response to covid-19 on access to healthcare for non-COVID-19 health issues in slum communities of Bangladesh, Kenya, Nigeria and Pakistan: Results of pre-COVID and COVID-19 lockdown stakeholder engagements. BMJ Glob. Heal. 5 , 1–17 (2020). CAS Google Scholar Rudenstine, S. et al. Examining the role of material and social assets on mental health in the context of COVID-19 among an urban public university sample. Psychol. Trauma Theory Res. Pract. Policy https://doi.org/10.1037/tra0001307 (2022). Gu, H. Y. & Wang, C. W. Impacts of the COVID-19 pandemic on vegetable production and countermeasures from an agricultural insurance perspective. J. Integr. Agric. 19 , 2866–2876 (2020). Dubey, S. et al. Psychosocial impact of COVID-19. Diabetes Metab. Syndr. Clin. Res. Rev. 14 , 779–788 (2020). Boughton, D. et al. Impacts of COVID-19 on agricultural production and food systems in late transforming Southeast Asia: The case of Myanmar. Agric. Syst. 188 , 103026 (2021). Talukder, B., VanLoon, G. W., Hipel, K. W. & Orbinski, J. COVID-19’s implications on agri-food systems and human health in Bangladesh. Curr. Res. Environ. Sustain. 3 , 100033 (2021). Alam, M. J. et al. The impact of the COVID-19 pandemic on vegetable farmers in Bangladesh. Cogent Food Agric. 9 , 2214432 (2023). Download references AcknowledgementsThe authors acknowledge the International Food Policy Research Institute (2022X020.BAU) and the Australian Centre for International Agricultural Research (ACIAR). The authors also wish to express their gratitude to Md Shajedur Rahaman, Senior Scientific Officer, Agricultural Economics Division, Bangladesh Rice Research Institute, for his assistance in generating the study area map. Author informationAuthors and affiliations. Department of Agribusiness and Marketing, Bangladesh Agricultural University, Mymensingh, 2202, Bangladesh Umme Salma, Mohammad Jahangir Alam, Tamanna Mastura & Md. Salauddin Palash Department of Agricultural Economics, Bangladesh Agricultural University, Mymensingh, 2202, Bangladesh Ismat Ara Begum School of Economics, Zhongnan University of Economics and Law, Wuhan, 430073, China Md Abdur Rouf Sarkar Agricultural Economics Division, Bangladesh Rice Research Institute, Gazipur, 1701, Bangladesh School of Agriculture, Food and Wine, The University of Adelaide, Adelaide, 5005, Australia Tamara Jackson Department of Agribusiness and Agricultural Economics, University of Arkansas, Fayetteville, AR, 72701, USA Andrew M. McKenzie Development Strategies and Governance Unit, International Food Policy Research Institute, New Delhi, 110012, India Avinash Kishore You can also search for this author in PubMed Google Scholar ContributionsU.S.: Conceived and designed the experiments; Performed the experiments; Analyzed and interpreted the data; Wrote the paper. M.J.A.; I.A.B.: Conceived and designed the experiments; Analyzed and interpreted the data; Wrote the paper. M.A.R.S.; T.J.; T.M.: Conceived and designed the experiments; Contributed reagents, materials, analysis tools, or data; Wrote the paper. M.S.P.; A.M.M.; A.K.: Analyzed and interpreted the data; Wrote the paper. Corresponding authorCorrespondence to Mohammad Jahangir Alam . Ethics declarationsCompeting interests. The authors declare no competing interests. Additional informationPublisher's note. Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations. Supplementary InformationSupplementary information 1., supplementary information 2., rights and permissions. Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/ . Reprints and permissions About this articleCite this article. Salma, U., Alam, M.J., Begum, I.A. et al. The impact of COVID-19 on livelihood assets: a case study of high-value crop farmers in North-West Bangladesh. Sci Rep 14 , 20121 (2024). https://doi.org/10.1038/s41598-024-71242-4 Download citation Received : 17 February 2024 Accepted : 26 August 2024 Published : 29 August 2024 DOI : https://doi.org/10.1038/s41598-024-71242-4 Share this articleAnyone you share the following link with will be able to read this content: Sorry, a shareable link is not currently available for this article. Provided by the Springer Nature SharedIt content-sharing initiative
By submitting a comment you agree to abide by our Terms and Community Guidelines . If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate. Quick links
Sign up for the Nature Briefing newsletter — what matters in science, free to your inbox daily.  | ||||||||||||||||
IMAGES
VIDEO
COMMENTS
CASE STUDY Mike (social anxiety) Case Study Details. Mike is a 20 year-old who reports to you that he feels depressed and is experiencing a significant amount of stress about school, noting that he'll "probably flunk out." He spends much of his day in his dorm room playing video games and has a hard time identifying what, if anything, is ...
Social anxiety disorder (SAD), also known as social phobia, is one of the most common anxiety disorders. ... In our case study, the duration of each session lasted 50 minutes and we gave 20 sessions of individual therapy to our client over a period of 5 months, thus trying to tailor our client's needs and requirements for treatment. ...
Treatment of Social Anxiety Disorder: A Case Study of an 11-Year-Old ...
This case study deals with Sara, a 37-year-old social phobic woman who suffered from a primary fear of blushing as well as comorbid disorders, including obsessive-compulsive disorder, generalized anxiety disorder and spider phobia. The client was treated in an intensive, one-week group cognitive-behavioral therapy program in an educational university clinic in Aarhus, Denmark.
Social Phobia/Anxiety Case Study: Jim. Jim was a nice looking man in his mid-30's. He could trace his shyness to boyhood and his social anxiety to his teenage years. He had married a girl he knew well from high school and had almost no other dating history. He and his wife, Lesley, had three children, two girls and a boy.
Sara, A Social Phobia Client with Sudden Change After Exposure Exercises in Intensive Cognitive-Behavior Group Therapy: A Case-Based Analysis of Mechanisms of Change. VICKI L. JENSEN a, ESBEN HOUGAARD a,c, & DANIEL B. FISHMAN b. Department of Psychology and Behavioural Sciences, University of Aarhus, Denmark.
Analysis and Insights. Sarah's case study offers valuable insights into the treatment of social anxiety disorder and highlights several key factors contributing to her success: 1. Comprehensive approach: The combination of psychotherapy, medication, and exposure techniques addressed multiple aspects of Sarah's anxiety.
Guided by the cognitive behavior therapy (CBT) (Beck, 2020) framework, the therapist approached Gi's case with special attention to the interpretations, assumptions, and beliefs that seemed to maintain his social anxiety.The way Gi saw himself and others' views of him seemed to be informed by a deeply held belief that "I am incompetent" and an expectation that others are critical and ...
This aligns with the pre- to post-intervention progress shown by Josie (using the Reliable Change Index), particularly in measures assessing acceptance, psychological inflexibility, and self-reported social anxiety. Josie's case study gives preliminary evidence of the acceptability and feasibility of the ACT@TeenSAD, making it a helpful tool ...
The 2013 updated NICE guideline, Social Anxiety Disorder: Recognition, Assessment and Treatment, has been critically reviewed and applied to a case study. The guideline is intended to provide evidence-based best practice advice for providers on how to recognize, complete assessments of, and treat social anxiety disorder.
Abstract. A case report is presented of Penny, aged 28, who was referred to the psychology pathway in the chronic pain service after reporting feeling anxious and low during a physiotherapy appointment for neck pain. An initial assessment highlighted Penny experienced anxiety in social situations and had a pervasive low mood stemming from her ...
Social anxiety disorder (previously termed 'social phobia') was formally recognised as a separate phobic disorder in the mid-1960s (Marks & Gelder, 1965). The term 'social anxiety disorder' reflects current understanding, including in diagnostic manuals, and is used throughout the guideline. As set out in the International Classification of Diseases, 10th Revision (ICD-10) (World ...
Social anxiety disorder (SAD), also known as social phobia, is one of the most common anxiety disorders and has been shown to be effectively treated using cognitive-behavioral therapy (CBT). ... The cognitive-behavioral treatment of social phobia. Clinical Case Studies. 2004; 3:124-146. [Google Scholar] Gould RA, Buckminster S, Pollack MH ...
After his first therapy session, Williams began his road to recovery. "After I was diagnosed with social anxiety disorder, I felt immense relief because it meant that there was a name for my suffering. I wasn't crazy or weird, like I thought for so many years," said Williams. "As part of my treatment program, my physician prescribed an ...
Emotional and behavioral symptoms. Signs and symptoms of social anxiety disorder can include constant: Fear of situations in which you may be judged negatively. Worry about embarrassing or humiliating yourself. Intense fear of interacting or talking with strangers. Fear that others will notice that you look anxious.
Abstract. Chapter 8 covers the treatment of Social Anxiety Disorder (SAD), and includes information about the condition, epidemiological considerations, the case study, assessment strategy and case formulation, intervention model and course of treatment, strategies for handling homework non-compliance, handling poor attendance and relapse, relapse prevention, post-treatment assessment, basic ...
Social Anxiety Disorder (SAD) is defined as an intense fear or anxiety associated with exposure to social scrutiny in past, current, or future social situations. Social situations might involve interactions (e.g., having a conversation with someone familiar or a stranger), being observed (e.g., while eating or writing), or performing in front ...
Counselling Case Study: Social Anxiety. Sasha is a 60 year old woman who has recently retired from a career in teaching. Working for many years in a secondary school environment, Sasha was confident, motivated and dedicated to her work, but at the same time looking forward to retirement so she and her husband could travel and spend more time ...
Case Study 1: Overcoming Social Anxiety. Case Study 2: Triumphing Over Panic Attacks. Case Study 3: Mastering Generalised Anxiety. Common Themes and Strategies. The Role of Resilience. Inspiring Others. Anxiety is a formidable adversary in the everyday life of many people in the UK. According to statistics, around 6% of people are diagnosed ...
Sir, Social phobias come under the category of phobic anxiety disorders and are centered around a fear of scrutiny by other people, usually leading to avoidance of social situations.[] Although social anxiety has been found to be the most common comorbidity in people with psychosis,[] social phobia or anxiety per se is a neurotic disorder in which the patient usually maintains an adequate ...
Introduction. Anxiety disorders affect as many as 30% of children and adolescents and contribute to social and academic dysfunction. These disorders or their temperamental precursors1 are often evident in early childhood, with 10% of children ages 2-5 already exhibiting anxiety disorders.2 Anxiety symptoms in toddlerhood3 and preschool age4 show moderate persistence and map on to the ...
CASE STUDY A CASE STUDY OF SOCIAL PHOBIA: SELF-PERCEPTION OF BEING UGLY Saliha Anjum GC University, Lahore This case study discusses the case of a 21 years old young man referred be-cause of his problem of social anxiety and strong feelings of ugliness. The cli-ent fulfilled the DSM-IV-TR criteria of Social Phobia. His family background
Hannah, an anxious child. This article presents a case study of an anxious child, and highlights some common symptoms for parents and teachers to be watchful for. The case study involves a fictitious identity; any resemblance to a real person is completely coincidental. Hannah (not a real person) was a 10-year-old girl from a close, supportive ...
The COVID-19 pandemic caused widespread disruption and increased concerns about mental health. One area of particular concern is social anxiety disorder (SAD), as the lockdowns and restrictions have made it difficult for people to engage in social activities. Studies show inconsistency in the prevalence rates reported in different studies, making it difficult to draw a clear picture of the ...
Alopecia areata (AA), or hair loss on the scalp and body, affects approximately 1 in 1,000 people. Psychological distress has been hypothesized as a determining factor of AA. Researchers evaluating psychological disorders in the development and course of AA have found equivocal results. Furthermore, few studies have evaluated parental distress in relation to childhood AA. Case studies have ...
The uncertainty and health risks posed by the epidemic increased the prevalence of depression and anxiety. Farmers grappled with the social and economic consequences, which led to heightened ...