Fact sheets
- Facts in pictures
- Publications
- Questions and answers
- Tools and toolkits
- Endometriosis
- Excessive heat
- Mental disorders
- Polycystic ovary syndrome
- All countries
- Eastern Mediterranean
- South-East Asia
- Western Pacific
- Data by country
- Country presence
- Country strengthening
- Country cooperation strategies
- News releases
- Feature stories
- Press conferences
- Commentaries
- Photo library
- Afghanistan
- Cholera
- Coronavirus disease (COVID-19)
- Greater Horn of Africa
- Israel and occupied Palestinian territory
- Disease Outbreak News
- Situation reports
- Weekly Epidemiological Record
- Surveillance
- Health emergency appeal
- International Health Regulations
- Independent Oversight and Advisory Committee
- Classifications
- Data collections
- Global Health Observatory
- Global Health Estimates
- Mortality Database
- Sustainable Development Goals
- Health Inequality Monitor
- Global Progress
- World Health Statistics
- Partnerships
- Committees and advisory groups
- Collaborating centres
- Technical teams
- Organizational structure
- Initiatives
- General Programme of Work
- WHO Academy
- Investment in WHO
- WHO Foundation
- External audit
- Financial statements
- Internal audit and investigations
- Programme Budget
- Results reports
- Governing bodies
- World Health Assembly
- Executive Board
- Member States Portal
- Fact sheets /

Cardiovascular diseases (CVDs)
- Cardiovascular diseases (CVDs) are the leading cause of death globally.
- An estimated 17.9 million people died from CVDs in 2019, representing 32% of all global deaths. Of these deaths, 85% were due to heart attack and stroke.
- Over three quarters of CVD deaths take place in low- and middle-income countries.
- Out of the 17 million premature deaths (under the age of 70) due to noncommunicable diseases in 2019, 38% were caused by CVDs.
- Most cardiovascular diseases can be prevented by addressing behavioural and environmental risk factors such as tobacco use, unhealthy diet and obesity, physical inactivity, harmful use of alcohol and air pollution.
- It is important to detect cardiovascular disease as early as possible so that management with counselling and medicines can begin.
Cardiovascular diseases (CVDs) are a group of disorders of the heart and blood vessels. They include:
- coronary heart disease – a disease of the blood vessels supplying the heart muscle;
- cerebrovascular disease – a disease of the blood vessels supplying the brain;
- peripheral arterial disease – a disease of blood vessels supplying the arms and legs;
- rheumatic heart disease – damage to the heart muscle and heart valves from rheumatic fever, caused by streptococcal bacteria;
- congenital heart disease – birth defects that affect the normal development and functioning of the heart caused by malformations of the heart structure from birth; and
- deep vein thrombosis and pulmonary embolism – blood clots in the leg veins, which can dislodge and move to the heart and lungs.
Heart attacks and strokes are usually acute events and are mainly caused by a blockage that prevents blood from flowing to the heart or brain. The most common reason for this is a build-up of fatty deposits on the inner walls of the blood vessels that supply the heart or brain. Strokes can be caused by bleeding from a blood vessel in the brain or from blood clots.
What are the risk factors for cardiovascular disease?
The most important behavioural risk factors of heart disease and stroke are unhealthy diet, physical inactivity, tobacco use and harmful use of alcohol. Amongst environmental risk factors, air pollution is an important factor. The effects of behavioural risk factors may show up in individuals as raised blood pressure, raised blood glucose, raised blood lipids, and overweight and obesity. These “intermediate risks factors” can be measured in primary care facilities and indicate an increased risk of heart attack, stroke, heart failure and other complications.
Cessation of tobacco use, reduction of salt in the diet, eating more fruit and vegetables, regular physical activity and avoiding harmful use of alcohol have been shown to reduce the risk of cardiovascular disease. Health policies that create conducive environments for making healthy choices affordable and available, as well as improving air quality and reducing pollution, are essential for motivating people to adopt and sustain healthy behaviours.
There are also a number of underlying determinants of CVDs. These are a reflection of the major forces driving social, economic and cultural change – globalization, urbanization and population ageing. Other determinants of CVDs include poverty, stress and hereditary factors.
In addition, drug treatment of hypertension, diabetes and high blood lipids are necessary to reduce cardiovascular risk and prevent heart attacks and strokes among people with these conditions.
What are common symptoms of cardiovascular diseases?
Symptoms of heart attacks and strokes.
Often, there are no symptoms of the underlying disease of the blood vessels. A heart attack or stroke may be the first sign of underlying disease. Symptoms of a heart attack include:
- pain or discomfort in the centre of the chest; and/or
- pain or discomfort in the arms, the left shoulder, elbows, jaw, or back.
In addition the person may experience difficulty in breathing or shortness of breath; nausea or vomiting; light-headedness or faintness; a cold sweat; and turning pale. Women are more likely than men to have shortness of breath, nausea, vomiting, and back or jaw pain.
The most common symptom of a stroke is sudden weakness of the face, arm, or leg, most often on one side of the body. Other symptoms include sudden onset of:
- numbness of the face, arm, or leg, especially on one side of the body;
- confusion, difficulty speaking or understanding speech;
- difficulty seeing with one or both eyes;
- difficulty walking, dizziness and/or loss of balance or coordination;
- severe headache with no known cause; and/or
- fainting or unconsciousness.
People experiencing these symptoms should seek medical care immediately.
What is rheumatic heart disease?
Rheumatic heart disease is caused by damage to the heart valves and heart muscle from the inflammation and scarring caused by rheumatic fever. Rheumatic fever is caused by an abnormal response of the body to infection with streptococcal bacteria, which usually begins as a sore throat or tonsillitis in children.
Rheumatic fever mostly affects children in developing countries, especially where poverty is widespread. Globally, about 2% of deaths from cardiovascular diseases are related to rheumatic heart disease.
Symptoms of rheumatic heart disease
Symptoms of rheumatic heart disease include: shortness of breath, fatigue, irregular heartbeats, chest pain and fainting.
Symptoms of rheumatic fever include: fever, pain and swelling of the joints, nausea, stomach cramps and vomiting.
Why are cardiovascular diseases a development issue in low- and middle-income countries?
At least three-quarters of the world's deaths from CVDs occur in low- and middle-income countries. People living in low- and middle-income countries often do not have the benefit of primary health care programmes for early detection and treatment of people with risk factors for CVDs. People in low- and middle-income countries who suffer from CVDs and other noncommunicable diseases have less access to effective and equitable health care services which respond to their needs. As a result, for many people in these countries detection is often late in the course of the disease and people die at a younger age from CVDs and other noncommunicable diseases, often in their most productive years.
The poorest people in low- and middle-income countries are most affected. At the household level, evidence is emerging that CVDs and other noncommunicable diseases contribute to poverty due to catastrophic health spending and high out-of-pocket expenditure. At the macro-economic level, CVDs place a heavy burden on the economies of low- and middle-income countries.
How can the burden of cardiovascular diseases be reduced?
The key to cardiovascular disease reduction lies in the inclusion of cardiovascular disease management interventions in universal health coverage packages, although in a high number of countries health systems require significant investment and reorientation to effectively manage CVDs.
Evidence from 18 countries has shown that hypertension programmes can be implemented efficiently and cost-effectively at the primary care level which will ultimately result in reduced coronary heart disease and stroke. Patients with cardiovascular disease should have access to appropriate technology and medication. Basic medicines that should be available include:
- beta-blockers;
- angiotensin-converting enzyme inhibitors; and
An acute event such as a heart attack or stroke should be promptly managed.
Sometimes, surgical operations are required to treat CVDs. They include:
- coronary artery bypass;
- balloon angioplasty (where a small balloon-like device is threaded through an artery to open the blockage);
- valve repair and replacement;
- heart transplantation; and
- artificial heart operations.
Medical devices are required to treat some CVDs. Such devices include pacemakers, prosthetic valves, and patches for closing holes in the heart.
WHO response
In 2013, WHO Member States agreed on global mechanisms to reduce the avoidable NCD burden including a "Global action plan for the prevention and control of NCDs 2013-2020". This Plan aims to reduce the number of premature deaths from NCDs by 25% by 2025 through nine voluntary global targets. Two of the targets directly focus on preventing and controlling CVDs.
Target 6: Reduce global prevalence of raised blood pressure by 25% between 2010 and 2025.
Target 8: At least 50% of eligible people should receive drug therapy and counselling (including glycaemic control) to prevent heart attacks and strokes by 2025.
In addition, target 9 states that there should be 80% availability of the affordable basic technologies and essential medicines, including generics, required to treat major NCDs in both public and private facilities.
Achieving these targets will require significant investment in and strengthening of health systems.
WHO is currently working on increasing the normative guidance available for the management of acute coronary syndrome and stroke which will provide guidance in these important areas.
Related links
- Global action plan for the prevention and control of NCDs 2013-2020
- Health topic: cardiovascular diseases
Overview of Coronary Artery Disease
- Pathophysiology |
- Risk Factors |
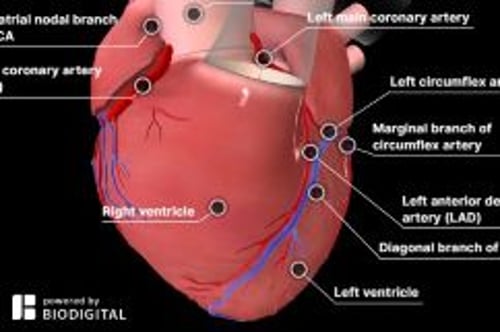
- Coronary Artery Anatomy |
- Treatment |
- Prevention |
Coronary artery disease (CAD) involves impairment of blood flow through the coronary arteries, most commonly by atheromas. Clinical presentations include silent ischemia, angina pectoris , acute coronary syndromes ( unstable angina , myocardial infarction ), and sudden cardiac death . Diagnosis is by symptoms, ECG, stress testing, and sometimes coronary angiography. Prevention consists of modifying reversible risk factors (eg, hypercholesterolemia, hypertension, physical inactivity, obesity, diabetes, smoking). Treatment includes medications and procedures to reduce ischemia and restore or improve coronary blood flow.
Coronary artery disease is the leading cause of death in both sexes, accounting for approximately one third of all deaths, and substantial numbers of these occur in low resource areas ( 1 ). Mortality from coronary artery disease is approximately 5 times higher in men than in women, but the mortality difference declines with age ( 2 ).
General references
1. Ralapanawa U, Sivakanesan R . Epidemiology and the Magnitude of Coronary Artery Disease and Acute Coronary Syndrome: A Narrative Review. J Epidemiol Glob Health 2021;11(2):169-177. doi:10.2991/jegh.k.201217.001
2. Bots SH, Peters SAE, Woodward M . Sex differences in coronary heart disease and stroke mortality: a global assessment of the effect of ageing between 1980 and 2010. BMJ Glob Health 2017;2(2):e000298. Published 2017 Mar 27. doi:10.1136/bmjgh-2017-000298
Etiology of Coronary Artery Disease
Usually, coronary artery disease is due to
Coronary artery atherosclerosis : Subintimal deposition of atheromas in large and medium-sized coronary arteries
Less often, coronary artery disease is due to
Coronary artery spasm (see Vasospastic Angina )
Vascular endothelial dysfunction can promote atherosclerosis and contribute to coronary artery spasm. Endothelial dysfunction is also recognized as a cause of angina in the absence of epicardial coronary artery stenosis or spasm (see Microvascular Angina ).
Rare causes include coronary artery embolism, dissection, aneurysm (eg, in Kawasaki disease ), and vasculitis (eg, in Takayasu arteritis ).
Pathophysiology of Coronary Artery Disease
Coronary atherosclerosis.
Coronary atherosclerosis is often irregularly distributed in different vessels but typically occurs at points of turbulence (eg, vessel bifurcations). As the atheromatous plaque grows, the arterial lumen progressively narrows, resulting in ischemia (often causing angina pectoris ). The degree of stenosis required to cause ischemia varies with oxygen demand.
Occasionally, an atheromatous plaque ruptures or splits. Reasons are unclear but probably relate to plaque morphology, plaque calcium content, and plaque softening due to an inflammatory process. Rupture exposes collagen and other thrombogenic material, which activate platelets and the coagulation cascade (see figure Pathways in Blood Coagulation ), resulting in an acute thrombus, which interrupts coronary blood flow and causes some degree of myocardial ischemia. The consequences of acute ischemia, collectively referred to as acute coronary syndromes (ACS), depend on the location and degree of obstruction and range from unstable angina, non–ST-segment elevation myocardial infarction (NSTEMI), to ST-segment elevation myocardial infarction (STEMI), which can result in transmural infarction, and other complications including malignant ventricular arrhythmias, conduction defects, heart failure, and sudden death.
Coronary artery spasm
Coronary artery spasm is a transient, focal increase in vascular tone, markedly narrowing the lumen and reducing blood flow; symptomatic ischemia ( vasospastic angina ) may result. Marked narrowing can trigger thrombus formation, causing infarction or life-threatening arrhythmia. Spasm can occur in arteries with or without atheroma.
In arteries without atheroma, basal coronary artery tone is probably increased, and response to vasoconstricting stimuli is probably exaggerated. The exact mechanism is unclear but may involve endothelial cell abnormalities of nitric oxide production or an imbalance between endothelium-derived contracting and relaxing factors.
In arteries with atheroma, the atheroma causes endothelial dysfunction, possibly resulting in local hypercontractility. Proposed mechanisms include loss of sensitivity to intrinsic vasodilators (eg, acetylcholine) and increased production of vasoconstrictors (eg, angiotensin II , endothelin, leukotrienes, serotonin, thromboxane) in the area of the atheroma. Recurrent spasm may damage the intima, leading to atheroma formation.
Use of vasoconstricting substances (eg, cocaine , nicotine ) and emotional stress also can trigger coronary spasm.
Coronary artery dissection
Coronary artery dissection is a rare, non-traumatic tear in the coronary intima with creation of a false lumen. Blood flowing through the false lumen expands it, which restricts blood flow through the true lumen sometimes causing coronary ischemia or infarction. Dissection may occur in atherosclerotic or non-atherosclerotic coronary arteries. Non-atherosclerotic dissection is more likely in pregnant or postpartum females and/or patients with fibromuscular dysplasia or other connective tissue disorders.
Risk Factors for Coronary Artery Disease
Risk factors for coronary artery disease are the same as risk factors for atherosclerosis :
Family history of early coronary artery disease (death from coronary artery disease in a first-degree relative prior to age 55 in males or age 65 in females)
High blood levels of low-density lipoprotein (LDL) cholesterol (see Dyslipidemia )
High blood levels of lipoprotein a
Low blood levels of high-density lipoprotein (HDL) cholesterol
Diabetes mellitus (particularly type 2)
Smoking (including secondhand exposure)
Physical inactivity
High level of apoprotein B (apo B)
High blood levels of C-reactive protein (CRP)
Smoking may be a stronger predictor of myocardial infarction in females ( 1 ). Genetic factors play a role, and several systemic disorders (eg, hypertension , hypothyroidism ) and metabolic disorders (eg, hyperhomocysteinemia ) contribute to risk. A high level of apo B may identify increased risk when total cholesterol or LDL level is normal ( 2, 3 ).
High blood levels of C-reactive protein indicate plaque instability and inflammation and may be a stronger predictor of risk of ischemic events than high levels of LDL ( 4 ). High blood levels of triglycerides and insulin (reflecting insulin resistance) may be risk factors, but data are less clear. CAD risk is also increased by a diet high in fat and calories and low in phytochemicals (found in fruits and vegetables), fiber, and vitamins C, D, and E; by a diet relatively low in omega-3 (n-3) polyunsaturated fatty acids (PUFAs—at least in some people); and by poor stress management.
Risk factor references
1. Prescott E, Hippe M, Schnohr P, Hein HO, Vestbo J . Smoking and risk of myocardial infarction in women and men: longitudinal population study. BMJ 1998;316(7137):1043-1047. doi:10.1136/bmj.316.7137.1043
2. Sniderman AD, Thanassoulis G, Glavinovic T, et al . Apolipoprotein B Particles and Cardiovascular Disease: A Narrative Review. JAMA Cardiol 2019 Dec 1;4(12):1287-1295. doi: 10.1001/jamacardio.2019.3780
3. Wilkins JT, Li RC, Sniderman A, Chan C, Lloyd-Jones DM . Discordance Between Apolipoprotein B and LDL-Cholesterol in Young Adults Predicts Coronary Artery Calcification: The CARDIA Study. J Am Coll Cardiol 2016;67(2):193-201. doi:10.1016/j.jacc.2015.10.055
4. Ridker PM, Lei L, Louie MJ, et al . Inflammation and Cholesterol as Predictors of Cardiovascular Events Among 13 970 Contemporary High-Risk Patients With Statin Intolerance. Circulation 2024;149(1):28-35. doi:10.1161/CIRCULATIONAHA.123.066213
Coronary Artery Anatomy
The right and left coronary arteries arise from the right and left coronary sinuses in the root of the aorta just above the aortic valve orifice (see figure Arteries of the Heart ). The coronary arteries divide into large and medium-sized arteries that run along the heart’s surface (epicardial coronary arteries) and subsequently send smaller arterioles into the myocardium.
The left coronary artery begins as the left main artery and quickly divides into the left anterior descending (LAD), circumflex, and sometimes an intermediate artery (ramus intermedius). The LAD artery usually follows the anterior interventricular groove and, in some people, continues over the apex. This artery supplies the anterior septum (including the proximal conduction system) and the anterior free wall of the left ventricle (LV). The circumflex artery, which is usually smaller than the LAD artery, supplies the lateral LV free wall.
The dominant coronary artery refers to the one that gives rise to the posterior descending artery. Most people have right dominance: The right coronary artery passes along the atrioventricular (AV) groove over the right side of the heart; it supplies the sinus node (in 55%), right ventricle, and usually the AV node and inferior myocardial wall. About 10 to 15% of people have left dominance: The circumflex artery is larger and continues along the posterior AV groove to supply the posterior wall and AV node.
Arteries of the Heart
|
Treatment of Coronary Artery Disease
Medical therapy, including antiplatelet agents, lipid-lowering drugs (eg, statins), and beta-blockers
Percutaneous coronary intervention (PCI)
For acute thrombosis, sometimes fibrinolytic drugs
Coronary artery bypass grafting (CABG)
Treatment generally aims to reduce cardiac workload by decreasing oxygen demand and improving coronary artery blood flow, and, over the long term, to halt and reverse the atherosclerotic process. Coronary artery blood flow can be improved by percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG). An acute coronary thrombosis may sometimes be dissolved by fibrinolytic drugs .
Medical therapy
(See also Medications for Acute Coronary Syndromes .)
Medical management of patients with CAD depends on symptoms, cardiac function, and the presence of other disorders. Recommended therapy includes
Antiplatelet agents to prevent thrombus formation
Statins to lower LDL cholesterol levels
Beta-blockers to reduce symptoms of angina
Antiplatelet agents and statins improve short-term and long-term outcomes, probably by improving atheromatous plaque stability and endothelial function.
Beta-blockers reduce symptoms of angina by reducing heart rate and contractility and decreasing myocardial oxygen demand. Beta-blockers also reduce mortality post-infarction, especially in the presence of post-myocardial infarction (MI) LV dysfunction.
Calcium channel blockers are also helpful. They often are combined with beta-blockers in managing angina and hypertension but have not been proven to reduce mortality.
Nitrates modestly dilate coronary arteries and decrease venous return, decreasing cardiac work and relieving angina quickly. Longer acting nitrate formulations help decrease angina events but do not decrease mortality.
Angiotensin-converting enzyme (ACE) inhibitors and angiotensin II receptor blockers (ARBs) are most effective at reducing mortality post MI in CAD patients with LV dysfunction ( 1, 2 ).
Little evidence exists to guide therapy for patients with endothelial dysfunction. Treatment is generally similar to that for typical large-vessel atherosclerosis, and some evidence suggests that use of beta-blockers may enhance endothelial function ( 3 ).
(See Percutaneous Coronary Interventions .)
PCI is indicated for patients with acute coronary syndrome (ACS) or with stable ischemic heart disease who have angina despite optimal medical therapy.
Drug-eluting stents, < 10% ( 4 ). Most PCI is done with stents, and most stents used in the United States are drug-eluting.
Patients without significant infarct or complications may return to work and usual activities usually within a few days after stent placement. However, cardiac rehabilitation is recommended for all patients.
In-stent thrombosis occurs because of the inherent thrombogenicity of metallic stents. Most cases occur within the first 24 to 48 hours. However, late stent thrombosis, occurring after 30 days and as late as ≥ 1 year (rarely), can occur with both bare-metal and drug-eluting stents, especially after cessation of antiplatelet therapy. Progressive endothelialization of the bare-metal stent occurs within the first few months and reduces the risk of thrombosis. However, the antiproliferative drugs released by drug-eluting stents inhibit this process and prolong the risk of thrombosis. Thus, patients who undergo stent placement are treated with various antiplatelet agents . The current standard regimen for patients with a bare-metal or drug-eluting stent consists of all of the following ( 5 ):
Glycoprotein IIb/IIIa inhibitors are not routinely used in stable patients (ie, no comorbidities, no acute coronary syndrome) having elective stent placement. They may be beneficial in some patients with an acute coronary syndrome but should not be considered routine. It is unclear whether it is beneficial to give glycoprotein IIb/IIIa inhibitors before arrival in the cardiac catheterization laboratory, but most national organizations do not recommend their use in this situation ( 5 ).
A statin is started after stent insertion, if one is not already being used because PCI by itself does not cure or prevent the progression of CAD. Statin therapy has been shown to improve long-term event-free survival ( 6 ). Patients who receive a statin before the procedure have a lower risk of periprocedural MI.
Overall, risks of undergoing PCI are comparable to those of CABG. Overall mortality rate is < 1%, but varies based on individual risk factors and tends to be similar to that of CABG; Q wave MI rate is < 1%. In < 1% of patients, intimal dissection causes obstruction requiring emergency CABG. Risk of stroke with PCI is lower than with CABG. A meta-analysis of 19 randomized trials reported a higher risk of stroke in patients undergoing CABG (1.2%) than PCI (0.34%,) at 30 days ( 7 ). Risk of bleeding is 1 to 2%.
(See Coronary Artery Bypass Grafting .)
CABG uses arteries (eg, internal mammary, radial) whenever possible, and if necessary, sections of autologous veins (eg, saphenous) to bypass diseased segments of the coronary arteries. At 1 year, about 85% of venous bypass grafts are patent, and after 5 years, one third or more are completely blocked. However, after 10 years, as many as 97% of internal mammary artery grafts are patent ( 8 ). Arteries also hypertrophy to accommodate increased flow. CABG is superior to PCI in patients with diabetes and in patients with multivessel disease amenable to grafting.
Coronary artery bypass grafting is typically done during cardiopulmonary bypass with the heart stopped; a bypass machine pumps and oxygenates blood. Risks of the procedure include stroke and MI. For patients with a normal-sized heart, no history of MI, good ventricular function, and no additional risk factors, risk is < 5% for perioperative MI, 1 to 2% for stroke, and ≤ 1% for mortality; risk increases with age, poor LV function, and presence of underlying disease. Operative mortality rate is 3 to 5 times higher for a second bypass than for the first.
After cardiopulmonary bypass, about 25 to 30% of patients develop cognitive dysfunction or behavioral changes, possibly caused by microemboli originating in the bypass machine ( 9 ). Cognitive or behavioral changes are more prevalent in older patients, prompting suspicion that these changes are most likely due to diminished "neuronal reserve," making older patients more susceptible to minor injuries incurred during cardiopulmonary bypass. Dysfunction ranges from mild to severe and may persist for weeks to years. To minimize this risk, some centers use a beating heart technique (off-pump CABG, which uses no cardiopulmonary bypass), in which a device mechanically stabilizes the part of the heart upon which the surgeon is working. However, long-term studies have failed to demonstrate lasting benefits of this approach in comparison to conventional on-pump CABG.
CAD may progress despite bypass surgery. Postoperatively, the rate of proximal obstruction of bypassed vessels increases. Vein grafts become obstructed early if thrombi form and later (several years) if atherosclerosis causes slow degeneration of the intima and media. Aspirin prolongs vein graft patency. Continued smoking has a profound adverse effect on patency. After CABG, a statin should be started or continued at maximally tolerated doses.
Treatment references
1. Indications for ACE inhibitors in the early treatment of acute myocardial infarction: systematic overview of individual data from 100,000 patients in randomized trials. ACE Inhibitor Myocardial Infarction Collaborative Group. Circulation 1998;97(22):2202-2212. doi:10.1161/01.cir.97.22.2202
2. Düsing R . Mega clinical trials which have shaped the RAS intervention clinical practice. Ther Adv Cardiovasc Dis 2016;10(3):133-150. doi:10.1177/1753944716644131
3. Peller M, Ozierański K, Balsam P, Grabowski M, Filipiak KJ, Opolski G . Influence of beta-blockers on endothelial function: A meta-analysis of randomized controlled trials. Cardiol J 2015;22(6):708-716. doi:10.5603/CJ.a2015.0042
4. Bønaa KH, Mannsverk J, Wiseth R, et al . Drug-Eluting or Bare-Metal Stents for Coronary Artery Disease. N Engl J Med 2016;375(13):1242-1252. doi:10.1056/NEJMoa1607991
5. Writing Committee Members, Lawton JS, Tamis-Holland JE, et al . 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines [published correction appears in J Am Coll Cardiol 2022 Apr 19;79(15):1547]. J Am Coll Cardiol 2022;79(2):e21-e129. doi:10.1016/j.jacc.2021.09.006
6. Grundy SM, Stone NJ, Bailey AL, et al : 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines [published correction appears in Circulation 2019 Jun 18;139(25):e1182-e1186] [published correction appears in Circulation 2023 Aug 15;148(7):e5]. Circulation 139(25):e1082–e1143, 2019. doi:10.1161/CIR.0000000000000625
7. Palmerini T, Biondi-Zoccai G, Reggiani LB, et al : Risk of stroke with coronary artery bypass graft surgery compared with percutaneous coronary intervention. J Am Coll Cardiol 60(9):798–805, 2012. doi:10.1016/j.jacc.2011.10.912
8. Hillis LD, Smith PK, Anderson JL, et al : 2011 ACCF/AHA Guideline for Coronary Artery Bypass Graft Surgery: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines [published correction appears in Circulation 2011 Dec 20;124(25):e957]. Circulation 124(23):e652–e735, 2011. doi:10.1161/CIR.0b013e31823c074e
9. Kulik A, Ruel M, Jneid H, et al : Secondary prevention after coronary artery bypass graft surgery: a scientific statement from the American Heart Association. Circulation 131(10):927–964, 2015. doi:10.1161/CIR.0000000000000182
Prevention of Coronary Artery Disease
The American Heart Association (AHA) recommends using the pooled cohort risk assessment equations to estimate lifetime and 10-year risk of atherosclerotic cardiovascular disease. The risk calculator is based on sex, age, race, total and high-density lipoprotein (HDL) cholesterol levels, systolic blood pressure (and whether blood pressure is being treated), diabetes, and smoking status ( 1 ).
Prevention of coronary artery disease involves modifying atherosclerosis risk factors :
Smoking cessation
Weight loss
Healthful diet
Regular exercise
Modification of serum lipid levels
Reduction of salt intake
Control of hypertension
Control of diabetes
Antihypertensive recommendations vary. In the United States, for patients who are at low risk ( < 10% 10-year risk) of atherosclerotic cardiovascular disease (ASCVD), antihypertensive therapy is recommended if blood pressure is > 130/80. In patients with coronary artery disease or whose risk of ASCVD is > 10%, antihypertensive medication is recommended for blood pressure > 130/80 mm Hg ( 2 ).
Modification of serum lipid levels (particularly with statins) may slow or even partially reverse the progression of CAD. Treatment goals have been modified. Instead of trying to achieve specific target low-density lipoprotein (LDL) cholesterol levels, patients are selected for treatment based on their risk of ASCVD. Lower risk patients with elevated LDL may not require statin treatment. Four higher risk patient groups have been identified in whom the benefit of statin therapy outweighs the risk of adverse events:
Patients with clinical ASCVD
Patients with LDL cholesterol ≥ 190 mg/dL ( ≥ 4.9 mmol/L)
Patients age 40 to 75 years with diabetes and LDL cholesterol levels of 70 to 189 mg/dL (1.8 to 4.9 mmol/L)
Patients age 40 to 75 years without diabetes, with LDL cholesterol levels of 70 to 189 mg/dL (1.8 to 4.9 mmol/L), and with ASCVD risk > 7.5%
Nicotinic acid or a fibrate may be added for patients with an HDL cholesterol level < 40 mg/dL ( < 1.03 mmol/L), although several trials have failed to demonstrate a lower risk of ischemia or slowed progression of atherosclerosis when medications are used to raise HDL ( 3 ).
≥ 60 years ( 4 ). It can be considered for patients aged 40 to 59 years whose 10-year risk of cardiovascular disease exceeds 10%, but absolute benefit is likely to be small.
Prevention references
1. Arnett DK, Blumenthal RS, Albert MA, et al : 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 74:1376–1414, 2019. doi: 10.1016/j.jacc.2019.03.009
2. Whelton PB, Carey RM, Aronow WS, et al : ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 71:e127–e248, 2018. doi: 10.1161/HYP.0000000000000066
3. AIM-HIGH Investigators, Boden WE, Probstfield JL, Anderson T, et al : Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy. N Engl J Med 365(24): 2255–2267, 2011. doi: 10.1056/NEJMoa1107579
4. US Preventive Services Task Force, Davidson KW, Barry MJ, et al : Aspirin Use to Prevent Cardiovascular Disease: US Preventive Services Task Force Recommendation Statement. JAMA 327(16):1577–1584, 2022. doi:10.1001/jama.2022.4983

Copyright © 2024 Merck & Co., Inc., Rahway, NJ, USA and its affiliates. All rights reserved.
- Cookie Preferences

- Patient Care & Health Information
- Diseases & Conditions
- Coronary artery disease
- Coronary artery disease FAQs
Mayo Clinic cardiologist Stephen Kopecky, M.D., answers the most frequently asked questions about coronary artery disease (CAD).
Hi, I'm Dr. Steve Kopecky, a cardiologist at Mayo Clinic. And I'm here to answer some of the important questions you may have about coronary artery disease.
Many small changes can lead to great benefit over time. Remember that nothing you do to improve your health is ever too little. And nothing you do to improve your health is ever too late.
Cholesterol is always involved in the initiation of the narrowing of the arteries to the heart. And every plaque or narrowing of your arteries contains cholesterol. It is essential to control the cholesterol in order to optimally lower your chance of a heart attack.
Yes. All the studies that have shown regression of arterial narrowing have done three things. First, take care of the obvious factors like high blood pressure, smoking and high cholesterol. Second, address diet and physical activity. And third, help patients manage stress.
No. Half of the time, the first symptom a person has of coronary artery disease is actually a heart attack. And half of these heart attacks are fatal. So overall, for one out of four people, the first symptom is what we term sudden cardiac death.
No. Studies have shown that even if your cholesterol is well control with medicines, if you do not eat a healthy diet, your heart attack, stroke, and death rate is not significantly reduced.
Yes. Since your heart beats one hundred thousand times a day, even mild elevations of blood pressure above 130 over 80 can cause significant health problems, including heart attacks, strokes and heart failure.
I tell people they have a new part-time job called Your Health. In part of this is knowing what medicines you're on, what doses you're taking and why you're taking these medicines. Also very helpful, check your blood pressure regularly. Check your weight regularly at home. If any questions arise about your health, put them in your smartphone, so you'll have them the next time you have your visit with your doctor. Never hesitate to ask your medical team any questions or concerns you have. Being informed makes all the difference. Thanks for your time and we wish you well.
To diagnose coronary artery disease, a healthcare professional examines you. You are usually asked questions about your medical history and any symptoms. If you have symptoms of coronary artery disease such as chest pain or shortness of breath, tests may be done to check your overall health.
Tests to help diagnose or watch coronary artery disease include:
- Blood tests. Blood tests can check blood sugar and cholesterol levels. A high-sensitivity C-reactive protein (CRP) test checks for a protein linked to inflammation of the arteries.
- Electrocardiogram (ECG or EKG). This quick test checks the electrical activity of the heart. It shows how the heart is beating. Sticky patches called electrodes attach to the chest and sometimes the arms and legs. Wires connect the electrodes to a computer, which prints or displays the test results. The ECG signal patterns can show if you had or are having a heart attack.
- Echocardiogram. This test uses sound waves to show blood flow through the heart. Parts of the heart that move weakly may be caused by a lack of oxygen or a heart attack. This may be a sign of coronary artery disease or other conditions.
- Exercise stress test. If your symptoms usually occur during exercise, your healthcare professional may recommend this test. You walk on a treadmill or ride a stationary bike while your heart is checked. Because exercise makes the heart pump harder and faster than it does during most daily activities, an exercise stress test can show heart problems that might otherwise be missed. If you can't exercise, you may be given a medicine that affects the heart like exercise does. Sometimes an echocardiogram is done during an exercise stress test.
- Nuclear stress test. This test shows how blood moves to the heart at rest and during activity. It uses a small amount of radioactive material, called a tracer or radiotracer. The substance is given by IV. An imaging machine takes pictures of how the tracer moves through the heart arteries. This helps find areas of poor blood flow or heart damage.
- Heart CT scan. A CT scan of the heart can show calcium deposits and blockages in the heart arteries. Calcium deposits can narrow the arteries. Sometimes dye is given by IV during this test. The dye helps create detailed pictures of the heart arteries. If dye is used, the test is called a CT coronary angiogram.
- Cardiac catheterization and angiogram. This test can see blockages in the heart arteries. A doctor places a long, thin flexible tube called a catheter in a blood vessel, usually in the groin or wrist. It's guided to the heart. Dye flows through the catheter to arteries in the heart. The dye helps the arteries show up more clearly on X-ray images and video. Heart treatments may be done during this test.
- Care at Mayo Clinic
Our caring team of Mayo Clinic experts can help you with your coronary artery disease-related health concerns Start Here
More Information
Coronary artery disease care at Mayo Clinic
- Cardiac catheterization
- Coronary angiogram
- Coronary calcium scan
- Echocardiogram
- Electrocardiogram (ECG or EKG)
- Stress test
Treatment for coronary artery disease may include:
- Lifestyle changes such as not smoking, eating healthy and exercising more.
- Heart procedure or heart surgery.
Medications
Many medicines are available to treat coronary artery disease, including:
- Cholesterol medicine. Your healthcare professional might recommend this type of medicine to lower "bad" LDL cholesterol and reduce plaque buildup in the arteries. Such medicines include statins, niacin, fibrates and bile acid sequestrants.
Aspirin. Aspirin helps thin the blood and prevent blood clots. Daily low-dose aspirin therapy may be recommended for the primary prevention of heart attack or stroke in some people.
Daily use of aspirin can have serious side effects, including bleeding in the stomach and intestines. Don't start taking a daily aspirin without talking to your healthcare team.
- Beta blockers. These medicines slow the heartbeat and lower blood pressure. If you've had a heart attack, beta blockers may reduce the risk of future heart attacks.
- Calcium channel blockers. One of these medicines may be suggested if you can't take beta blockers or beta blockers don't work for you. Calcium channel blockers can help reduce chest pain.
- Angiotensin-converting enzyme (ACE) inhibitors and angiotensin 2 receptor blockers (ARBs). These medicines lower blood pressure. They may help keep coronary artery disease from getting worse.
- Nitroglycerin. This medicine widens the heart arteries. It can help control or reduce chest pain. Nitroglycerin is available as a pill, spray or patch.
- Ranolazine. This medicine may help people with long-term chest pain. It may be prescribed with or instead of a beta blocker.
Surgeries or other procedures

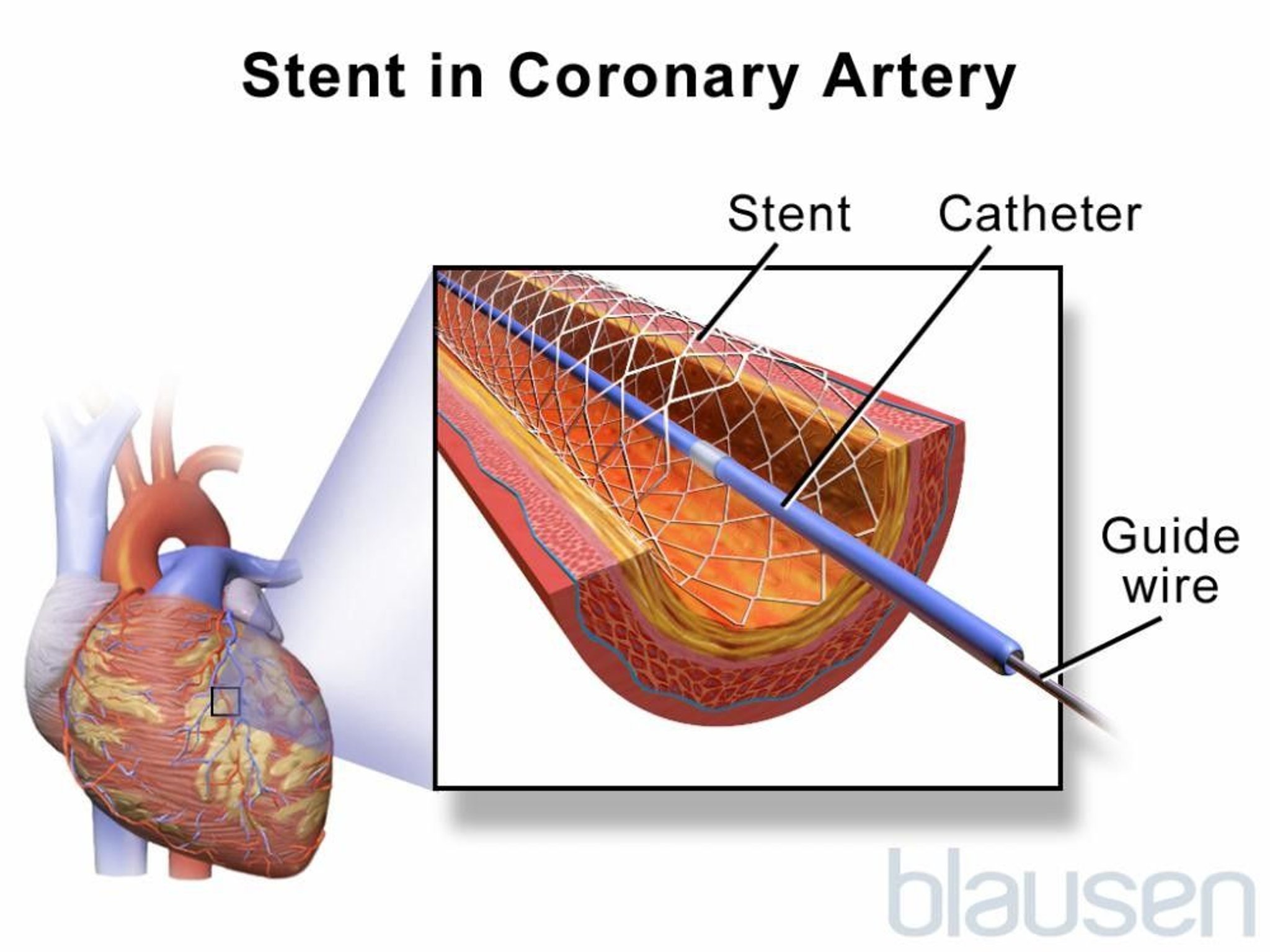
- Coronary artery stent
To place a coronary artery stent, a balloon on the tip of the catheter is inflated to widen the blocked artery (A). Then a metal mesh stent is placed (B). The stent helps hold the artery open so blood can flow through it (C).

- Coronary artery bypass surgery
Coronary artery bypass surgery creates a new path for blood to flow to the heart. A healthy blood vessel from another part of the body is used to redirect blood around a blocked area of an artery. Usually the blood vessel is taken from an artery in the chest, called the internal mammary artery. Sometimes it's taken from a leg vein, called the saphenus vein.
Surgery may be done to fix a blocked artery and improve blood flow. Surgeries or procedures for coronary artery disease may include:
- Coronary angioplasty and stent placement. This treatment opens clogged blood vessels in the heart. A tiny balloon on a thin tube, called a catheter, is used to widen a clogged artery and improve blood flow. A small wire mesh tube called a stent may be placed to keep the artery open. Most stents are coated with medicine that helps keep the artery open. This treatment also is called percutaneous coronary intervention.
- Coronary artery bypass graft (CABG) surgery. This is a type of open-heart surgery. During CABG, a surgeon takes a vein or artery from somewhere else in the body. The surgeon uses the blood vessel to create a new path for blood to go around a blocked or narrowed heart artery. The surgery increases blood flow to the heart.
If you've had coronary artery bypass surgery, your healthcare professional may suggest cardiac rehabilitation. This is a program of education, counseling and exercise training that's designed to help improve your health after heart surgery.
- Angina treatment: Stents, drugs, lifestyle changes — What's best?
- Drug-eluting stents
- Coronary artery disease: Angioplasty or bypass surgery?
- Coronary angioplasty and stents
Clinical trials
Explore Mayo Clinic studies testing new treatments, interventions and tests as a means to prevent, detect, treat or manage this condition.
Alternative medicine
Omega-3 fatty acids are a type of unsaturated fatty acid. It's thought that they can lower inflammation throughout the body. Inflammation has been linked to coronary artery disease. However, the reasons for and against omega-3 fatty acids for heart disease continue to be studied.
Sources of omega-3 fatty acids include:
- Fish and fish oil. Fish and fish oil are the most effective sources of omega-3 fatty acids. Fatty fish — such as salmon, herring and light canned tuna — have the most omega-3 fatty acids. Fish oil supplements may offer benefit, but the evidence is strongest for eating fish.
- Flax and flaxseed oil. Flax and flaxseed oil contain a type of omega-3 fatty acid called alpha-linolenic acid (ALA). ALA contains smaller amounts of omega-3 fatty acids than do fish and fish oil. ALA may help lower cholesterol and improve heart health. But research is mixed. Some studies haven't found flax and flaxseed oil to be as effective as fish. Flaxseed also contains a lot of fiber, which has various health benefits.
- Other oils. Alpha-linolenic acid (ALA) also can be found in canola oil, soybeans and soybean oil.
Other supplements and food items may help lower blood pressure or cholesterol — two risk factors for coronary artery disease. Some that may work are:
- Psyllium, a type of fiber.
- Oats, a type of fiber that includes beta-glucans and is found in oatmeal and whole oats.
- Plant sterols, found in supplements and some margarines, such as Promise, Smart Balance and Benecol.
Always talk to a healthcare professional before taking herbs, supplements or medicines bought without a prescription.
Lifestyle and home remedies
Making certain lifestyle changes can help keep the arteries healthy and can prevent or slow coronary artery disease. Try these heart-healthy tips:
- Don't smoke or use tobacco. Smoking is a major risk factor for coronary artery disease. Nicotine tightens blood vessels and forces the heart to work harder. Not smoking is one of the best ways to lower the risk of a heart attack. If you need help quitting, talk to your healthcare team.
- Eat heart-healthy foods. Choose plenty of fruits, vegetables and whole grains. Limit sugar, salt and saturated fats. Eating one or two servings of fish a week also may help keep the heart healthy.
- Get regular exercise. Exercise helps manage weight and control diabetes, cholesterol and blood pressure — all risk factors for coronary artery disease. Try to get 30 to 60 minutes of physical activity most days of the week. Ask your healthcare team what amount and type of exercise is best for you.
- Keep a healthy weight. Being overweight increases the risk of coronary artery disease. Losing even a small amount of weight can help reduce risk factors for coronary artery disease. Ask your healthcare team what the best weight is for you.
- Control blood pressure. Adults should get their blood pressure checked by a healthcare professional at least every two years. You may need to have checks more often if you have a history of high blood pressure. Ask your health professional what blood pressure goal is best for you.
- Get your cholesterol checked. Ask your healthcare team how often you need a cholesterol test. Lifestyle changes and medicines may be recommended to control cholesterol.
- Check your blood sugar. If you have diabetes, carefully managing your blood sugar can help reduce the risk of coronary artery disease.
- Avoid or limit alcohol. If you choose to drink alcohol, do so in moderation. For healthy adults, that means up to one drink a day for women and up to two drinks a day for men.
- Get good sleep. Poor sleep may increase the risk of heart disease and other chronic conditions. Adults should aim to get 7 to 9 hours of sleep daily.
- Manage stress. Find ways to help reduce emotional stress. Getting more exercise, practicing mindfulness and connecting with others in support groups are some ways to reduce stress.
Regular health checkups also are important. Some of the main risk factors for coronary artery disease — high cholesterol, high blood pressure and diabetes — have no symptoms in the early stages. Early detection and treatment can help you keep your heart healthy. Also ask about recommended vaccines, such as a yearly flu vaccine.
The lifestyle habits used to treat coronary artery disease also can help prevent it. A healthy lifestyle can help keep the arteries strong and clear of blockages. To improve heart health, follow these tips:
- Do not smoke or use tobacco.
- Limit or do not drink alcohol.
- Control blood pressure, cholesterol and diabetes.
- Exercise and stay active.
- Maintain a healthy weight.
- Eat a low-fat, low-salt diet that's rich in fruits, vegetables and whole grains.
- Reduce and manage stress.
- Get 7 to 9 hours of sleep daily.
Preparing for your appointment
If you have symptoms of coronary artery disease or any risk factors, make an appointment for a health checkup. You may be sent to a doctor trained in heart diseases, called a cardiologist.
Here's some information to help you get ready for your appointment.
What you can do
- Be aware of any pre-appointment restrictions. When you make the appointment, ask if there's anything you need to do in advance, such as restrict your diet. For example, you may be told not to eat or drink for a few hours before a cholesterol test.
- Write down any symptoms you're having, including any that may seem unrelated to coronary artery disease.
- Write down your medical information, including other conditions you have and any family history of heart disease.
- Bring a list of medicines with you to your appointment. Include doses.
- Ask a family member or friend to go with you to the appointment, if possible. An extra person can help you remember details from the appointment..
- Write down questions to ask your healthcare team.
Questions to ask your healthcare professional at your first appointment include:
- What is causing my symptoms?
- What tests do I need?
- Should I see a specialist?
- Do I need to change my activity or diet while I wait for my next appointment?
- When should I call 911 or emergency medical help for my symptoms?
If you're sent to a cardiologist for coronary artery disease, you may want to ask these questions:
- What is my risk of long-term complications from coronary artery disease?
- What treatment do you recommend?
- If I need medicine, what are the possible side effects?
- Do I need surgery? Why or why not?
- What diet and lifestyle changes should I make?
- How often do I need follow-up visits?
- I have other health conditions. How can I best manage these conditions together?
Don't hesitate to ask additional questions.
What to expect from your doctor
A healthcare professional who sees you for coronary artery disease may ask:
- What are your symptoms?
- When did you begin having symptoms?
- Have the symptoms gotten worse over time?
- Do you have chest pain or difficulty breathing?
- If so, what does the chest pain feel like?
- Does exercise or activity make the symptoms worse?
- Does anyone in your family have a heart condition or high blood pressure?
- Have you been diagnosed with other health conditions?
- What medicines do you take?
- How much do you exercise in a typical week?
- What's your usual daily diet?
- Do you or did you smoke? How much? If you quit, when?
- Do you drink alcohol? How much?
What you can do in the meantime
It's never too early to make healthy lifestyle changes, such as quitting smoking, eating healthy foods and getting more exercise. These habits protect against coronary artery disease and its complications, including heart attack and stroke.
- Ferri FF. Coronary artery disease. In: Ferri's Clinical Advisor 2022. Elsevier; 2022. https://www.clinicalkey.com. Accessed March 8, 2022.
- Coronary heart disease. National Heart, Lung, and Blood Institute. https://www.nhlbi.nih.gov/health-topics/coronary-heart-disease. March 8, 2022.
- Usatine RP, et al., eds. Coronary artery disease. In: Color Atlas and Synopsis of Heart Failure. McGraw Hill; 2019.
- Wilson PWF. Overview of the possible risk factors for cardiovascular disease. https://www.uptodate.com/contents/search. Accessed March 8, 2022.
- Masjedi MS, et al. Effects of flaxseed on blood lipids in healthy and dyslipidemic subjects: A systematic review and meta-analysis of randomized controlled trials. Current Problems in Cardiology. 2021; doi:10.1016/j.cpcardiol.2021.100931.
- Riaz H, et al. Association between obesity and cardiovascular outcomes: A systematic review and meta-analysis of mendelian randomization studies. JAMA Network Open. 2018; doi:10.1001/jamanetworkopen.2018.3788.
- Physical Activity Guidelines for Americans. 2nd ed. U.S. Department of Health and Human Services. https://health.gov/our-work/physical-activity/current-guidelines. Accessed March 8, 2022.
- Your guide to lowering your cholesterol with therapeutic lifestyle changes (TLC). National Heart, Lung, and Blood Institute. https://www.nhlbi.nih.gov/health-topics/all-publications-and-resources/your-guide-lowering-cholesterol-therapeutic-lifestyle. Accessed March 24, 2022.
- Rethinking drinking. National Institute on Alcohol Abuse and Alcoholism. https://www.rethinkingdrinking.niaaa.nih.gov/. Accessed March 24, 2022.
- 2015-2020 Dietary Guidelines for Americans. U.S. Department of Health and Human Services and U.S. Department of Agriculture. https://health.gov/our-work/food-nutrition/2015-2020-dietary-guidelines/guidelines. Accessed March 24, 2022.
- Omega-3 supplements: In depth. National Center for Complementary and Integrative Health. https://www.nccih.nih.gov/health/omega3-supplements-in-depth. Accessed March 8, 2022.
- Lopez-Jimenez F (expert opinion). Mayo Clinic. May 9, 2024.
- Siscovick DS, et al. Omega-3 polyunsaturated fatty acid (fish oil) supplementation and the prevention of clinical cardiovascular disease: A science advisory from the American Heart Association. Circulation. 2017; doi:10.1161/CIR.0000000000000482.
- Barley. Natural Medicines. https://naturalmedicines.therapeuticresearch.com. Accessed March 24, 2022.
- Black psyllium. Natural Medicines. https://naturalmedicines.therapeuticresearch.com. Accessed March 24, 2022.
- Nimmagadda R. Allscripts EPSi. Mayo Clinic. April 10, 2024.
- Liao KP. Coronary artery disease in rheumatoid arthritis: Pathogenesis, risk factors, clinical manifestations, and diagnostic implications. https://www.uptodate.com/contents/search. Accessed March 8, 2022.
- What is coronary heart disease? National Heart, Lung, and Blood Institute. https://www.nhlbi.nih.gov/health-topics/coronary-heart-disease Accessed March 8, 2022.
- Kannam JP, et al. Chronic coronary syndrome: Overview of care. https://www.uptodate.com/contents/search. Accessed March 8, 2022.
- Arnett DK, et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019; doi:10.1161/CIR.0000000000000678.
- Aspirin use to prevent cardiovascular disease: Preventive medication. U.S. Preventive Services Task Force. https://www.uspreventiveservicestaskforce.org/uspstf/draft-recommendation/aspirin-use-to-prevent-cardiovascular-disease-preventive-medication. Accessed March 23, 2021.
- Zheng SL, et al. Association of aspirin use for primary prevention with cardiovascular events and bleeding events: A systematic review and meta-analysis. JAMA. 2019; doi:10.1001/jama.2018.20578.
- Cutlip D, et al. Revascularization in patients with stable coronary artery disease: Coronary artery bypass graft surgery versus percutaneous coronary intervention. https://www.uptodate.com/contents/search. Accessed March 24, 2022.
- Hypertension in Adults: Screening. U.S. Preventive Services Task Force. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/hypertension-in-adults-screening. Accessed March 24, 2022.
- How and when to have your cholesterol checked. U.S. Centers for Disease Control and Prevention. https://www.cdc.gov/cholesterol/checked.htm. Accessed March 24, 2022.
- Blond psyllium. Natural Medicines. https://naturalmedicines.therapeuticresearch.com. Accessed March 24, 2022.
- Oats. Natural Medicines. https://naturalmedicines.therapeuticresearch.com. Accessed March 24, 2022.
- Garlic. Natural Medicines. https://naturalmedicines.therapeuticresearch.com. Accessed March 24, 2022.
- Plant sterols. Natural Medicines. https://naturalmedicines.therapeuticresearch.com. Accessed March 24, 2022.
- Ashraf H, et al. Use of flecainide in stable coronary artery disease: An analysis of its safety in both nonobstructive and obstructive coronary artery disease. American Journal of Cardiovascular Drugs. 2021; doi:10.1007/s40256-021-00483-9.
- Ono M, et al. 10-year follow-up after revascularization in elderly patients with complex coronary artery disease. Journal of the American College of Cardiology. 2021; doi:10.1016/j.jacc.2021.04.016.
- Coyle M, et al. A critical review of chronic kidney disease as a risk factor for coronary artery disease. International Journal of Cardiology: Heart & Vasculature. 2021; doi:10.1016/j.ijcha.2021.100822.
- Mankad R (expert opinion). Mayo Clinic. May 9, 2024.
- Scientific Report of the 2020 Dietary Guidelines Advisory Committee. Alcoholic beverages. U.S. Department of Health and Human Services and U.S. Department of Agriculture. https://www.dietaryguidelines.gov/2020-advisory-committee-report. Accessed Feb. 1, 2024.
- Heart disease in women. American Heart Association. https://www.heart.org/en/health-topics/heart-attack/warning-signs-of-a-heart-attack/heart-attack-symptoms-in-women. May 8, 2024.
- Four Steps to Heart Health
- What is coronary artery disease? A Mayo Clinic cardiologist explains.
Associated Procedures
News from mayo clinic.
- Mayo Clinic Minute: Signs of coronary artery disease, how to reduce your risk Jan. 24, 2023, 04:15 p.m. CDT
- A History of Cancer, Coronary Artery Disease May Reduce Risk of Dementia Oct. 24, 2022, 02:45 p.m. CDT
Mayo Clinic in Rochester, Minnesota, has been recognized as one of the top Cardiology & Heart Surgery hospitals in the nation for 2024-2025 by U.S. News & World Report.
- Symptoms & causes
- Diagnosis & treatment
- Doctors & departments
Mayo Clinic does not endorse companies or products. Advertising revenue supports our not-for-profit mission.
- Opportunities
Mayo Clinic Press
Check out these best-sellers and special offers on books and newsletters from Mayo Clinic Press .
- Mayo Clinic on Incontinence - Mayo Clinic Press Mayo Clinic on Incontinence
- The Essential Diabetes Book - Mayo Clinic Press The Essential Diabetes Book
- Mayo Clinic on Hearing and Balance - Mayo Clinic Press Mayo Clinic on Hearing and Balance
- FREE Mayo Clinic Diet Assessment - Mayo Clinic Press FREE Mayo Clinic Diet Assessment
- Mayo Clinic Health Letter - FREE book - Mayo Clinic Press Mayo Clinic Health Letter - FREE book
5X Challenge
Thanks to generous benefactors, your gift today can have 5X the impact to advance AI innovation at Mayo Clinic.
- Type 2 Diabetes
- Heart Disease
- Digestive Health
- Multiple Sclerosis
- Diet & Nutrition
- Health Insurance
- Public Health
- Patient Rights
- Caregivers & Loved Ones
- End of Life Concerns
- Health News
- Thyroid Test Analyzer
- Doctor Discussion Guides
- Hemoglobin A1c Test Analyzer
- Lipid Test Analyzer
- Complete Blood Count (CBC) Analyzer
- What to Buy
- Editorial Process
- Meet Our Medical Expert Board
What Is Heart Disease?
Also Known as Cardiovascular Disease (CVD)
Types of Heart Disease
Living with heart disease.
- Next in Heart Disease Guide Symptoms of Heart Disease
"Heart disease ," or cardiovascular disease (CVD), is an umbrella term for conditions affecting the heart and blood vessels. Sometimes people are born with heart disease (known as congenital heart disease ), while in others, it develops over time, as in coronary artery disease (CAD).
CVD is a leading cause of death in the United States, and coronary artery disease is estimated to affect 18.2 million American adults. In 2020, CVD accounted for 697,000—or 1 in 5–deaths.
It is important to know the early signs and symptoms of heart disease and how it can be prevented and treated. This article will explain the types of heart disease, signs and symptoms, treatment options, and best practices for preventing heart disease.
Suriyapong Thongsawang / Getty Images
Heart disease refers to several distinct heart and blood (cardiovascular) conditions. Types of CVD include the following:
- Congenital heart disease occurs when people are born with defects in their heart structure.
- Coronary heart disease ( coronary artery disease ) is the most common type of heart disease; it's characterized by a buildup of plaque and hardening of artery walls ( atherosclerosis ), which disrupts blood flow.
- Heart attack ( myocardial infarction ) is often caused by CAD and occurs when blood flow is blocked, causing heart muscles to die.
- Heart failure is a form of heart disease characterized by the heart not pumping enough blood; the heart is still working but not well enough.
- Arrhythmia is an irregular heartbeat, which can impact your heart’s ability to pump enough blood; your heart may beat too fast ( tachycardia ), too slowly ( bradycardia ), or inconsistently.
- Valvular stenosis occurs when one or more of the four valves of the heart do not open all the way; this can cause regurgitation , when blood leaks backward because the valve is closed.
Heart Disease vs. Heart Failure
The terms “heart disease” and “heart failure” are often confused. The key difference between the two is that heart failure—when the heart can’t pump sufficient blood—is a type of heart disease. Heart disease refers to a broad range of cardiovascular diseases.
Heart Disease Symptoms: How Do You Know You Have It?
Heart disease represents a wide range of conditions, and its symptoms can vary; different types come with different signs. CVD can be asymptomatic, meaning many people live for months or years without symptoms. Often, the underlying issue is not identified until it starts causing complications.
The symptoms of heart attack, arrhythmia, and heart failure often include the following:
- Chest pain and discomfort ( angina )
- Pain in the upper back or neck
- Indigestion and heartburn
- Nausea, vomiting
- Shortness of breath
- Fluttering the chest ( palpitations )
- Swelling in the feet, ankles, legs, abdomen (belly and chest), or neck veins
- Syncope (passing out)
CVD presents differently based on sex. Researchers found if you're assigned female at birth and younger than 65, you're less likely to report chest pain.
Heart Disease Symptoms Are an Emergency
If you experience any CVD symptoms, get emergency medical help. Heart attack can cause the heart to stop ( cardiac arrest ) and can become fatal without prompt treatment.
Early Signs of Heart Disease
Since many people with CVD have the condition without knowing it, it can be crucial to identify the early warning signs. People may experience these warning signs for months before serious complications, such as heart attack, occur. Warning signs include:
- Tightness, squeezing, pressure, or pain in the chest
- Discomfort or tightness in the body, including one or both arms, back, neck, jaw
- Difficulty breathing and shortness of breath
- Cold sweats
- Nausea or vomiting
- Light-headedness
For heart failure, troubling signs include:
- Difficulty breathing
- Persistent cough, wheezing
- Swollen ankles, feet, or other body parts
- Fatigue, lack of energy
- Nausea and loss of appetite
- Impaired thinking, confusion, and difficulty remembering
- Increased heart rate, heart palpitations
What Causes Heart Disease?
Heart disease is caused by various factors depending on the type of heart disease.
Some people are born with structural problems with their heart and associated arteries, affecting the heart's ability to pump blood effectively.
The most common cause of heart disease is atherosclerosis , which causes plaque buildup and hardened arterial walls. It develops gradually over time and eventually restricts blood flow due to narrowing arteries.
In some cases, people experience blood vessel problems. For instance, they may not respond to signals that the body needs more oxygen (such as during physical activity) and dilate as they should. Arteries of the heart can cause them to tighten or close up, a condition called vasospasm .
Heart Disease Risk Factors
Various factors can increase your risk of developing heart disease. Certain populations and people with specific underlying diseases are at higher risk of developing heart disease.
Non-Modifiable
Non-modifiable risk factors include:
- Family history of early heart disease
Modifiable risk factors include:
- Smoking or consistent exposure to secondhand smoke
- Physical inactivity, lack of exercise
- Insufficient or irregular sleep, insomnia , or other sleep disorders
- Unhealthy diet, especially one high in saturated fats and refined carbohydrates
- Environment (e.g., pollution, work conditions, etc.)
Underlying Conditions
Heart disease risk is also raised if you have any of the following diseases or conditions:
- High blood pressure (hypertension)
- High levels of low-density lipoprotein (LDL) cholesterol (considered "bad" cholesterol)
- High levels of blood triglycerides
- Atherosclerosis
- Autoimmune inflammatory conditions, including Crohn’s disease , psoriasis, ulcerative colitis, and others
- Diabetes mellitus
- Chronic kidney disease
- Being overweight or having obesity
- Human immunodeficiency virus (HIV)
- Depression, anxiety, or other mental health conditions
- Metabolic syndrome (a group of symptoms that when occurring together contribute to heart disease, stroke, or type 2 diabetes)
How to Prevent Heart Disease
You can take steps to reduce your risk and prevent heart disease. Most involve modifying lifestyle factors, such as in the following ways, to improve your overall health:
- Eat a heart-healthy diet : Eat various fruits and vegetables, limit food high in saturated and trans fats and added sugar and salt, and minimize alcohol consumption.
- Exercise regularly : Aim for 150 minutes of light to moderate activity, such as cycling, walking, running, or swimming, each week.
- Quit smoking : Tobacco use increases your risk of heart disease. If you use tobacco, talk to a healthcare provider about options for quitting.
- Manage your weight : Excess weight can stress your heart and blood vessels.
- Get good sleep : Aim for seven to eight hours each night. Following a sleep schedule can help you improve your sleep quality.
- Monitor risk factors : Manage any underlying conditions that put you at more risk by taking prescribed medications or making lifestyle changes to manage diabetes , high blood pressure , and other risk factors.
How Is Heart Disease Diagnosed?
A healthcare provider will assess your symptoms, take a medical history, and determine your risk factors of heart disease. A CVD diagnosis also based on the results of tests and imaging techniques.
Depending on your symptoms, a healthcare provider may use one or more of the following methods to diagnose and evaluate heart disease:
- Blood tests : A provider may order a blood test to examine your cholesterol levels, triglycerides, blood glucose (sugar), and lipoproteins (a sign of inflammation), which are markers of heart disease.
- Imaging : Healthcare providers may use various imaging techniques, including electrocardiogram (ECG/EKG), cardiac magnetic resonance imaging (MRI), Cardiac positron-emission tomography (PET ), cardiac computed tomography (CT), coronary calcium scan, or coronary angiography to diagnose heart disease.
- Stress testing : During a stress test, a healthcare provider will perform a single photon emission computed tomography (SPECT) scan while you run on a treadmill or pedal on an exercise bike to see how well your heart works under stress.
- Stress echo : This test assesses your heart using an echocardiogram while you exercise.
Heart Disease Treatment
Treatment approaches to heart disease can involve lifestyle changes, medications, or surgery, depending on the type of heart disease you have.
Lifestyle Changes
Preventive measures for CVD are a significant component of standard treatment and may include:
- Changing your diet
- Boosting physical activity or incorporating exercise
- Quitting smoking
- Ensuring you are getting good sleep
- Stress management techniques, such as mindfulness, yoga, and others
Medications
Prescribed medications for heart disease focus on treating risk factors to prevent complications or reduce symptoms. Several classes are considered for CVD:
- Angiotensin-converting enzyme (ACE) inhibitors are drugs used to treat high blood pressure and heart failure. Examples include Lotensin (benazepril) and captopril.
- Beta-blockers like Lopressor (metoprolol) and Tenormin (atenolol) treat heart arrhythmia, prevent a second heart attack, and lower blood pressure.
- Antidiabetics are drugs used to reduce sugar levels in people with diabetes and include Jardiance (empagliflozin) , Invokana (canagliflozin), and Victoza (liraglutide). They also reduce the risk of complications if you have diabetes and heart disease.
- Nitrates , such as Nitrostat (nitroglycerin), dilate blood vessels to restore blood flow and treat CVD.
- Statins , such as Mevacor (lovastatin) and Livalo (pitavastatin) reduce the risk of heart disease and lower cholesterol. A provider may recommend a statin if you’re at higher risk or have diabetes.
- Non-statins like Zetia (ezetimibe) or Repatha (alirocumab), among others, manage cholesterol, while Lopid (gemfibrozil) or Lipofen (fenofibrate) treat high triglycerides.
Complementary and Alternative Medicine
Some people with heart disease use various complementary and alternative medicine (CAM) approaches alongside standard therapies. These include:
- Certain supplements
Talk to a healthcare provider before implementing these approaches.
Percutaneous Coronary Intervention
Percutaneous coronary intervention (PCI), or angioplasty with stent placement, is a way for healthcare providers to treat CVD by way of the arteries and involves using a minimally invasive technique to access blockages or obstructions and open them up. After the procedure, a stent—a mesh support tube—is implanted to prevent the artery from closing.
Coronary Artery Bypass Graft
During coronary artery bypass graft (CABG) , or bypass surgery, a surgeon uses healthy vessels from the chest wall to reroute blood flow in the heart. The newly attached vessels bypass the blockage. This therapy is typically reserved for more severe or extensive cases.
Myocardial Revascularization
When other surgeries for CVD are unsuccessful or not recommended, healthcare providers use myocardial revascularization to treat blood clots and blockages in the heart. Using lasers, these procedures create holes in the heart's walls to allow blood to move more easily from the left ventricle to the middle of the heart.
Managing heart disease can be challenging since it requires lifestyle changes and keeping up with medications and appointments. It’s important to know where to find support and what you can do to help manage your condition. Here are some tips:
- Talk to your provider : If you need help to improve your diet, incorporate exercise, or need additional support, seek your provider’s insight. They may be able to point you to helpful professionals, programs, and resources.
- Seek support from family and friends : Talk to your family and friends to help them understand what you are going through; don’t be afraid to enlist their help.
- Consider therapy : Working with a mental health professional in individual or group sessions may help you cope with your condition and teach you strategies to manage stress.
- Log your health : Keep track of your medications and any unusual symptoms; this information can be helpful for appointments.
- Find support online : There also are support groups for those living with heart disease. Social media pages and message boards can be vital sources of information and community.
- Advocacy organizations : Advocacy agencies, such as the American Heart Association , promote heart research.
Outlook for Heart Disease
Complications like heart attacks are much more dangerous the second or third time they occur, so it's crucial to be proactive about managing heart disease. One wide-ranging review found that nearly 50% of people readmitted to the hospital with a second heart attack within 90 days of a first died within five years.
However, managing risk factors, implementing healthy lifestyle habits, and taking your medication as prescribed can help you reduce your risk of future cardiac events or complications.
MedlinePlus. Heart diseases .
National Heart, Lung, and Blood Institute. What is coronary heart disease ?
Centers for Disease Control and Prevention. Heart disease facts .
American Heart Association. What is cardiovascular disease ?
National Heart, Lung, and Blood Institute. Coronary heart disease: symptoms .
Keteepe-Arachi T, Sharma S. Cardiovascular disease in women: understanding symptoms and risk factors . Eur Cardiol . 2017;12(1):10-13. doi:10.15420/ecr.2016:32:1
American Heart Association. Early signs of a heart attack .
American Heart Association. Heart failure: Signs and symptoms .
National Heart, Lung, and Blood Institute. Coronary heart disease: Causes and risk factors .
Centers for Disease Control and Prevention. Prevent heart disease .
National Heart, Lung, and Blood Institute. Stroke: Diagnosis .
National Heart, Lung, and Blood Institute. Coronary heart disease: Diagnosis .
National Heart, Lung, and Blood Institute. Coronary heart disease: Treatment .
Chow SL, Bozkurt B, Baker WL, et al. Complementary and alternative medicines in the management of heart failure: a scientific statement from the American Heart Association . Circulation . 2023;147(2). doi:10.1161/CIR.0000000000001110
Nair R, Johnson M, Kravitz K, et al. Characteristics and outcomes of early recurrent myocardial infarction after acute myocardial infarction . JAHA . 2021;10(16):e019270. doi:10.1161/JAHA.120.019270
National Heart, Lung, and Blood Institute. Coronary heart disease: treatment .
By Mark Gurarie Gurarie is a freelance writer and editor. He is a writing composition adjunct lecturer at George Washington University.
A .gov website belongs to an official government organization in the United States.
A lock ( ) or https:// means you've safely connected to the .gov website. Share sensitive information only on official, secure websites.
- About Heart Disease
- Risk Factors
- Heart Disease Facts
- Healthy People 2030
- Heart Disease Communications Toolkit
- Grady Implementation Guide
- Community-Clinical Linkages Health Equity Guide
- Emergency Medical Services (EMS) Home Rule State Law Fact Sheet
- EMS and Community Paramedicine
- Heart Valve Disease Toolkits
- American Heart Month Toolkits
- Healthy Eating Communications Kit
Related Topics:
- About Stroke
- About High Blood Pressure
- About Cholesterol
About Coronary Artery Disease (CAD)
- Coronary artery disease (CAD) is the most common type of heart disease in the United States.
- CAD is caused by plaque buildup in the walls of the arteries that supply blood to the heart.
Coronary artery disease (CAD) is the most common type of heart disease in the United States. It is sometimes called coronary heart disease or ischemic heart disease.
For some people, the first sign of CAD is a heart attack . You and your health care team may be able to help reduce your risk for CAD.

Angina , or chest pain and discomfort, is the most common symptom of CAD. Angina can happen when too much plaque builds up inside arteries, causing them to narrow. Narrowed arteries can cause chest pain because they can block blood flow to your heart muscle and the rest of your body.
For many people, the first clue that they have CAD is a heart attack . Symptoms of heart attack include
- Chest pain or discomfort (angina)
- Weakness, light-headedness, nausea (feeling sick to your stomach), or a cold sweat
- Pain or discomfort in the arms or shoulder
- Shortness of breath
Over time, CAD can weaken the heart muscle. This may lead to heart failure, a serious condition where the heart can't pump blood the way it should.
Risk factors
Overweight, physical inactivity, unhealthy eating, and smoking tobacco are risk factors for CAD. A family history of heart disease also increases your risk for CAD, especially a family history of having heart disease at an early age (50 or younger).
To find out your risk for CAD, your health care team may measure your blood pressure, blood cholesterol, and blood sugar levels.
Learn more about heart disease risk factors .
CAD is caused by plaque buildup in the walls of the arteries that supply blood to the heart (called coronary arteries) and other parts of the body.
Plaque is made up of deposits of cholesterol and other substances in the artery. Plaque buildup causes the inside of the arteries to narrow over time, which can partially or totally block the blood flow. This process is called atherosclerosis.
If you’re at high risk for heart disease or already have symptoms, your doctor can use several tests to diagnose CAD.
- Measures the electrical activity, rate, and regularity of your heartbeat.
- Uses ultrasound (special sound wave) to create a picture of the heart.
- Measures your heart rate while you walk on a treadmill. This helps to determine how well your heart is working when it has to pump more blood.
- Uses x-rays to create a picture of the heart, lungs, and other organs in the chest.
- Checks the inside of your arteries for blockage by inserting a thin, flexible tube through an artery in the groin, arm, or neck to reach the heart. Health care professionals can measure blood pressure within the heart and the strength of blood flow through the heart’s chambers as well as collect blood samples from the heart or inject dye into the arteries of the heart (coronary arteries).
- Monitors blockage and flow of blood through the coronary arteries. Uses X-rays to detect dye injected via cardiac catheterization.
- A computed tomography (CT) scan that looks in the coronary arteries for calcium buildup and plaque.
Treatment and recovery
What is cardiac rehabilitation and recovery.
Cardiac rehabilitation is an important program for anyone recovering from a heart attack, heart failure, or other heart problem that required surgery or medical care. In these people, cardiac rehab can help improve quality of life and can help prevent another cardiac event. Cardiac rehabilitation is a supervised program that includes
- Physical activity
- Education about healthy living, including healthy eating, taking medicine as prescribed, and ways to help you quit smoking
- Counseling to find ways to relieve stress and improve mental health
A team of people may help you through cardiac rehabilitation, including your health care team, exercise and nutrition specialists, physical therapists, and counselors or mental health professionals.
How can I be healthier if I have coronary artery disease?
If you have CAD, your health care team may suggest the following steps to help lower your risk for heart attack or worsening heart disease:
- Lifestyle changes, such as eating a healthier (lower sodium, lower fat) diet, increasing physical activity, reaching a healthy weight, and quitting smoking
- Medicines to treat risk factors for CAD, such as high cholesterol, high blood pressure, or an irregular heartbeat
- Surgical procedures to help restore blood flow to the heart
Heart Disease
Heart disease is the leading cause of death in the United States.
For Everyone
Public health.
COMMENTS
What is heart disease? The American Heart Association explains the various types of heart disease, also called coronary artery disease and coronary heart disease.
Overview Coronary artery disease (CAD) is a common type of heart disease. It affects the main blood vessels that supply blood to the heart, called the coronary arteries. In CAD, there is reduced blood flow to the heart muscle. A buildup of fats, cholesterol and other substances in and on the artery walls, a condition called atherosclerosis, usually causes coronary artery disease. The buildup ...
Learn how to prevent cardiovascular diseases with the latest evidence-based recommendations from the 2019 ACC/AHA Guideline.
WHO cardiovascular diseases fact sheet providing key facts and information on risk factors, symptoms, rheumatic heart disease, treatment and prevention, WHO response.
Coronary artery disease is the leading cause of death in both sexes, accounting for approximately one third of all deaths, and substantial numbers of these occur in low resource areas (1). Mortality from coronary artery disease is approximately 5 times higher in men than in women, but the mortality difference declines with age (2).
Learn about symptoms, causes and treatment of cardiovascular disease, a term describing a wide range of conditions that can affect the heart.
To diagnose coronary artery disease, a healthcare professional examines you. You are usually asked questions about your medical history and any symptoms. If you have symptoms of coronary artery disease such as chest pain or shortness of breath, tests may be done to check your overall health.
Heart disease describes many types of conditions that alter normal heart functioning. Learn how to prevent heart issues and treat diagnosed CVD.
Coronary artery disease (CAD) is the most common type of heart disease in the United States. It is sometimes called coronary heart disease or ischemic heart disease. For some people, the first sign of CAD is a heart attack. You and your health care team may be able to help reduce your risk for CAD. Coronary artery disease is caused by plaque ...
During the past decade, our understanding of the pathophysiology of coronary artery disease (CAD) has undergone a remarkable evolution. We review here how these advances have altered our concepts of and clinical approaches to both the chronic and acute phases of CAD. Previously considered a cholesterol storage disease, we currently view atherosclerosis as an inflammatory disorder. The ...
chapter 24 occlusive cardiovascular disorders. myocardial infarction. Click the card to flip 👆. RT ischemia. death of heart muscle. cells are permanently destroyed due to sudden partial or complete block of coronary artery. decreased cardiac blood supply. cardiac damage. increased HR = more 02 in demand.
3. Adults who are 40 to 75 years of age and are being evaluated for cardiovascular disease prevention should undergo 10-year atherosclerotic cardiovascular disease (ASCVD) risk estimation and have a clinician- patient risk discussion before starting on pharmacological therapy, such as antihypertensive therapy, a statin, or aspirin.
The heart is a vital organ that pumps large quantities of blood throughout the body, oxygenating the cells non-stop. The blood flows through the heart and its four chambers in a very specific order. When that order is disrupted, such as in atrial septal disorder, oxygenated and deoxygenated blood gets mixed, overwhelming the heart and the lungs, causing severe consequences. Any change in the ...
Case Study case study: cardiovascular disorders cardiovascular disorders keiser university cardiovascular calculate smoking history in terms of pack years. has
Alterations in Cardiovascular Peripheral Circulatory Disorders. Get a hint. What is the main function of the cardiovascular system? Click the card to flip 👆. To circulate blood. Click the card to flip 👆.