
Chapter 11. Interviewing
Introduction.
Interviewing people is at the heart of qualitative research. It is not merely a way to collect data but an intrinsically rewarding activity—an interaction between two people that holds the potential for greater understanding and interpersonal development. Unlike many of our daily interactions with others that are fairly shallow and mundane, sitting down with a person for an hour or two and really listening to what they have to say is a profound and deep enterprise, one that can provide not only “data” for you, the interviewer, but also self-understanding and a feeling of being heard for the interviewee. I always approach interviewing with a deep appreciation for the opportunity it gives me to understand how other people experience the world. That said, there is not one kind of interview but many, and some of these are shallower than others. This chapter will provide you with an overview of interview techniques but with a special focus on the in-depth semistructured interview guide approach, which is the approach most widely used in social science research.
An interview can be variously defined as “a conversation with a purpose” ( Lune and Berg 2018 ) and an attempt to understand the world from the point of view of the person being interviewed: “to unfold the meaning of peoples’ experiences, to uncover their lived world prior to scientific explanations” ( Kvale 2007 ). It is a form of active listening in which the interviewer steers the conversation to subjects and topics of interest to their research but also manages to leave enough space for those interviewed to say surprising things. Achieving that balance is a tricky thing, which is why most practitioners believe interviewing is both an art and a science. In my experience as a teacher, there are some students who are “natural” interviewers (often they are introverts), but anyone can learn to conduct interviews, and everyone, even those of us who have been doing this for years, can improve their interviewing skills. This might be a good time to highlight the fact that the interview is a product between interviewer and interviewee and that this product is only as good as the rapport established between the two participants. Active listening is the key to establishing this necessary rapport.
Patton ( 2002 ) makes the argument that we use interviews because there are certain things that are not observable. In particular, “we cannot observe feelings, thoughts, and intentions. We cannot observe behaviors that took place at some previous point in time. We cannot observe situations that preclude the presence of an observer. We cannot observe how people have organized the world and the meanings they attach to what goes on in the world. We have to ask people questions about those things” ( 341 ).
Types of Interviews
There are several distinct types of interviews. Imagine a continuum (figure 11.1). On one side are unstructured conversations—the kind you have with your friends. No one is in control of those conversations, and what you talk about is often random—whatever pops into your head. There is no secret, underlying purpose to your talking—if anything, the purpose is to talk to and engage with each other, and the words you use and the things you talk about are a little beside the point. An unstructured interview is a little like this informal conversation, except that one of the parties to the conversation (you, the researcher) does have an underlying purpose, and that is to understand the other person. You are not friends speaking for no purpose, but it might feel just as unstructured to the “interviewee” in this scenario. That is one side of the continuum. On the other side are fully structured and standardized survey-type questions asked face-to-face. Here it is very clear who is asking the questions and who is answering them. This doesn’t feel like a conversation at all! A lot of people new to interviewing have this ( erroneously !) in mind when they think about interviews as data collection. Somewhere in the middle of these two extreme cases is the “ semistructured” interview , in which the researcher uses an “interview guide” to gently move the conversation to certain topics and issues. This is the primary form of interviewing for qualitative social scientists and will be what I refer to as interviewing for the rest of this chapter, unless otherwise specified.

Informal (unstructured conversations). This is the most “open-ended” approach to interviewing. It is particularly useful in conjunction with observational methods (see chapters 13 and 14). There are no predetermined questions. Each interview will be different. Imagine you are researching the Oregon Country Fair, an annual event in Veneta, Oregon, that includes live music, artisan craft booths, face painting, and a lot of people walking through forest paths. It’s unlikely that you will be able to get a person to sit down with you and talk intensely about a set of questions for an hour and a half. But you might be able to sidle up to several people and engage with them about their experiences at the fair. You might have a general interest in what attracts people to these events, so you could start a conversation by asking strangers why they are here or why they come back every year. That’s it. Then you have a conversation that may lead you anywhere. Maybe one person tells a long story about how their parents brought them here when they were a kid. A second person talks about how this is better than Burning Man. A third person shares their favorite traveling band. And yet another enthuses about the public library in the woods. During your conversations, you also talk about a lot of other things—the weather, the utilikilts for sale, the fact that a favorite food booth has disappeared. It’s all good. You may not be able to record these conversations. Instead, you might jot down notes on the spot and then, when you have the time, write down as much as you can remember about the conversations in long fieldnotes. Later, you will have to sit down with these fieldnotes and try to make sense of all the information (see chapters 18 and 19).
Interview guide ( semistructured interview ). This is the primary type employed by social science qualitative researchers. The researcher creates an “interview guide” in advance, which she uses in every interview. In theory, every person interviewed is asked the same questions. In practice, every person interviewed is asked mostly the same topics but not always the same questions, as the whole point of a “guide” is that it guides the direction of the conversation but does not command it. The guide is typically between five and ten questions or question areas, sometimes with suggested follow-ups or prompts . For example, one question might be “What was it like growing up in Eastern Oregon?” with prompts such as “Did you live in a rural area? What kind of high school did you attend?” to help the conversation develop. These interviews generally take place in a quiet place (not a busy walkway during a festival) and are recorded. The recordings are transcribed, and those transcriptions then become the “data” that is analyzed (see chapters 18 and 19). The conventional length of one of these types of interviews is between one hour and two hours, optimally ninety minutes. Less than one hour doesn’t allow for much development of questions and thoughts, and two hours (or more) is a lot of time to ask someone to sit still and answer questions. If you have a lot of ground to cover, and the person is willing, I highly recommend two separate interview sessions, with the second session being slightly shorter than the first (e.g., ninety minutes the first day, sixty minutes the second). There are lots of good reasons for this, but the most compelling one is that this allows you to listen to the first day’s recording and catch anything interesting you might have missed in the moment and so develop follow-up questions that can probe further. This also allows the person being interviewed to have some time to think about the issues raised in the interview and go a little deeper with their answers.
Standardized questionnaire with open responses ( structured interview ). This is the type of interview a lot of people have in mind when they hear “interview”: a researcher comes to your door with a clipboard and proceeds to ask you a series of questions. These questions are all the same whoever answers the door; they are “standardized.” Both the wording and the exact order are important, as people’s responses may vary depending on how and when a question is asked. These are qualitative only in that the questions allow for “open-ended responses”: people can say whatever they want rather than select from a predetermined menu of responses. For example, a survey I collaborated on included this open-ended response question: “How does class affect one’s career success in sociology?” Some of the answers were simply one word long (e.g., “debt”), and others were long statements with stories and personal anecdotes. It is possible to be surprised by the responses. Although it’s a stretch to call this kind of questioning a conversation, it does allow the person answering the question some degree of freedom in how they answer.
Survey questionnaire with closed responses (not an interview!). Standardized survey questions with specific answer options (e.g., closed responses) are not really interviews at all, and they do not generate qualitative data. For example, if we included five options for the question “How does class affect one’s career success in sociology?”—(1) debt, (2) social networks, (3) alienation, (4) family doesn’t understand, (5) type of grad program—we leave no room for surprises at all. Instead, we would most likely look at patterns around these responses, thinking quantitatively rather than qualitatively (e.g., using regression analysis techniques, we might find that working-class sociologists were twice as likely to bring up alienation). It can sometimes be confusing for new students because the very same survey can include both closed-ended and open-ended questions. The key is to think about how these will be analyzed and to what level surprises are possible. If your plan is to turn all responses into a number and make predictions about correlations and relationships, you are no longer conducting qualitative research. This is true even if you are conducting this survey face-to-face with a real live human. Closed-response questions are not conversations of any kind, purposeful or not.
In summary, the semistructured interview guide approach is the predominant form of interviewing for social science qualitative researchers because it allows a high degree of freedom of responses from those interviewed (thus allowing for novel discoveries) while still maintaining some connection to a research question area or topic of interest. The rest of the chapter assumes the employment of this form.
Creating an Interview Guide
Your interview guide is the instrument used to bridge your research question(s) and what the people you are interviewing want to tell you. Unlike a standardized questionnaire, the questions actually asked do not need to be exactly what you have written down in your guide. The guide is meant to create space for those you are interviewing to talk about the phenomenon of interest, but sometimes you are not even sure what that phenomenon is until you start asking questions. A priority in creating an interview guide is to ensure it offers space. One of the worst mistakes is to create questions that are so specific that the person answering them will not stray. Relatedly, questions that sound “academic” will shut down a lot of respondents. A good interview guide invites respondents to talk about what is important to them, not feel like they are performing or being evaluated by you.
Good interview questions should not sound like your “research question” at all. For example, let’s say your research question is “How do patriarchal assumptions influence men’s understanding of climate change and responses to climate change?” It would be worse than unhelpful to ask a respondent, “How do your assumptions about the role of men affect your understanding of climate change?” You need to unpack this into manageable nuggets that pull your respondent into the area of interest without leading him anywhere. You could start by asking him what he thinks about climate change in general. Or, even better, whether he has any concerns about heatwaves or increased tornadoes or polar icecaps melting. Once he starts talking about that, you can ask follow-up questions that bring in issues around gendered roles, perhaps asking if he is married (to a woman) and whether his wife shares his thoughts and, if not, how they negotiate that difference. The fact is, you won’t really know the right questions to ask until he starts talking.
There are several distinct types of questions that can be used in your interview guide, either as main questions or as follow-up probes. If you remember that the point is to leave space for the respondent, you will craft a much more effective interview guide! You will also want to think about the place of time in both the questions themselves (past, present, future orientations) and the sequencing of the questions.
Researcher Note
Suggestion : As you read the next three sections (types of questions, temporality, question sequence), have in mind a particular research question, and try to draft questions and sequence them in a way that opens space for a discussion that helps you answer your research question.
Type of Questions
Experience and behavior questions ask about what a respondent does regularly (their behavior) or has done (their experience). These are relatively easy questions for people to answer because they appear more “factual” and less subjective. This makes them good opening questions. For the study on climate change above, you might ask, “Have you ever experienced an unusual weather event? What happened?” Or “You said you work outside? What is a typical summer workday like for you? How do you protect yourself from the heat?”
Opinion and values questions , in contrast, ask questions that get inside the minds of those you are interviewing. “Do you think climate change is real? Who or what is responsible for it?” are two such questions. Note that you don’t have to literally ask, “What is your opinion of X?” but you can find a way to ask the specific question relevant to the conversation you are having. These questions are a bit trickier to ask because the answers you get may depend in part on how your respondent perceives you and whether they want to please you or not. We’ve talked a fair amount about being reflective. Here is another place where this comes into play. You need to be aware of the effect your presence might have on the answers you are receiving and adjust accordingly. If you are a woman who is perceived as liberal asking a man who identifies as conservative about climate change, there is a lot of subtext that can be going on in the interview. There is no one right way to resolve this, but you must at least be aware of it.
Feeling questions are questions that ask respondents to draw on their emotional responses. It’s pretty common for academic researchers to forget that we have bodies and emotions, but people’s understandings of the world often operate at this affective level, sometimes unconsciously or barely consciously. It is a good idea to include questions that leave space for respondents to remember, imagine, or relive emotional responses to particular phenomena. “What was it like when you heard your cousin’s house burned down in that wildfire?” doesn’t explicitly use any emotion words, but it allows your respondent to remember what was probably a pretty emotional day. And if they respond emotionally neutral, that is pretty interesting data too. Note that asking someone “How do you feel about X” is not always going to evoke an emotional response, as they might simply turn around and respond with “I think that…” It is better to craft a question that actually pushes the respondent into the affective category. This might be a specific follow-up to an experience and behavior question —for example, “You just told me about your daily routine during the summer heat. Do you worry it is going to get worse?” or “Have you ever been afraid it will be too hot to get your work accomplished?”
Knowledge questions ask respondents what they actually know about something factual. We have to be careful when we ask these types of questions so that respondents do not feel like we are evaluating them (which would shut them down), but, for example, it is helpful to know when you are having a conversation about climate change that your respondent does in fact know that unusual weather events have increased and that these have been attributed to climate change! Asking these questions can set the stage for deeper questions and can ensure that the conversation makes the same kind of sense to both participants. For example, a conversation about political polarization can be put back on track once you realize that the respondent doesn’t really have a clear understanding that there are two parties in the US. Instead of asking a series of questions about Republicans and Democrats, you might shift your questions to talk more generally about political disagreements (e.g., “people against abortion”). And sometimes what you do want to know is the level of knowledge about a particular program or event (e.g., “Are you aware you can discharge your student loans through the Public Service Loan Forgiveness program?”).
Sensory questions call on all senses of the respondent to capture deeper responses. These are particularly helpful in sparking memory. “Think back to your childhood in Eastern Oregon. Describe the smells, the sounds…” Or you could use these questions to help a person access the full experience of a setting they customarily inhabit: “When you walk through the doors to your office building, what do you see? Hear? Smell?” As with feeling questions , these questions often supplement experience and behavior questions . They are another way of allowing your respondent to report fully and deeply rather than remain on the surface.
Creative questions employ illustrative examples, suggested scenarios, or simulations to get respondents to think more deeply about an issue, topic, or experience. There are many options here. In The Trouble with Passion , Erin Cech ( 2021 ) provides a scenario in which “Joe” is trying to decide whether to stay at his decent but boring computer job or follow his passion by opening a restaurant. She asks respondents, “What should Joe do?” Their answers illuminate the attraction of “passion” in job selection. In my own work, I have used a news story about an upwardly mobile young man who no longer has time to see his mother and sisters to probe respondents’ feelings about the costs of social mobility. Jessi Streib and Betsy Leondar-Wright have used single-page cartoon “scenes” to elicit evaluations of potential racial discrimination, sexual harassment, and classism. Barbara Sutton ( 2010 ) has employed lists of words (“strong,” “mother,” “victim”) on notecards she fans out and asks her female respondents to select and discuss.
Background/Demographic Questions
You most definitely will want to know more about the person you are interviewing in terms of conventional demographic information, such as age, race, gender identity, occupation, and educational attainment. These are not questions that normally open up inquiry. [1] For this reason, my practice has been to include a separate “demographic questionnaire” sheet that I ask each respondent to fill out at the conclusion of the interview. Only include those aspects that are relevant to your study. For example, if you are not exploring religion or religious affiliation, do not include questions about a person’s religion on the demographic sheet. See the example provided at the end of this chapter.
Temporality
Any type of question can have a past, present, or future orientation. For example, if you are asking a behavior question about workplace routine, you might ask the respondent to talk about past work, present work, and ideal (future) work. Similarly, if you want to understand how people cope with natural disasters, you might ask your respondent how they felt then during the wildfire and now in retrospect and whether and to what extent they have concerns for future wildfire disasters. It’s a relatively simple suggestion—don’t forget to ask about past, present, and future—but it can have a big impact on the quality of the responses you receive.
Question Sequence
Having a list of good questions or good question areas is not enough to make a good interview guide. You will want to pay attention to the order in which you ask your questions. Even though any one respondent can derail this order (perhaps by jumping to answer a question you haven’t yet asked), a good advance plan is always helpful. When thinking about sequence, remember that your goal is to get your respondent to open up to you and to say things that might surprise you. To establish rapport, it is best to start with nonthreatening questions. Asking about the present is often the safest place to begin, followed by the past (they have to know you a little bit to get there), and lastly, the future (talking about hopes and fears requires the most rapport). To allow for surprises, it is best to move from very general questions to more particular questions only later in the interview. This ensures that respondents have the freedom to bring up the topics that are relevant to them rather than feel like they are constrained to answer you narrowly. For example, refrain from asking about particular emotions until these have come up previously—don’t lead with them. Often, your more particular questions will emerge only during the course of the interview, tailored to what is emerging in conversation.
Once you have a set of questions, read through them aloud and imagine you are being asked the same questions. Does the set of questions have a natural flow? Would you be willing to answer the very first question to a total stranger? Does your sequence establish facts and experiences before moving on to opinions and values? Did you include prefatory statements, where necessary; transitions; and other announcements? These can be as simple as “Hey, we talked a lot about your experiences as a barista while in college.… Now I am turning to something completely different: how you managed friendships in college.” That is an abrupt transition, but it has been softened by your acknowledgment of that.
Probes and Flexibility
Once you have the interview guide, you will also want to leave room for probes and follow-up questions. As in the sample probe included here, you can write out the obvious probes and follow-up questions in advance. You might not need them, as your respondent might anticipate them and include full responses to the original question. Or you might need to tailor them to how your respondent answered the question. Some common probes and follow-up questions include asking for more details (When did that happen? Who else was there?), asking for elaboration (Could you say more about that?), asking for clarification (Does that mean what I think it means or something else? I understand what you mean, but someone else reading the transcript might not), and asking for contrast or comparison (How did this experience compare with last year’s event?). “Probing is a skill that comes from knowing what to look for in the interview, listening carefully to what is being said and what is not said, and being sensitive to the feedback needs of the person being interviewed” ( Patton 2002:374 ). It takes work! And energy. I and many other interviewers I know report feeling emotionally and even physically drained after conducting an interview. You are tasked with active listening and rearranging your interview guide as needed on the fly. If you only ask the questions written down in your interview guide with no deviations, you are doing it wrong. [2]
The Final Question
Every interview guide should include a very open-ended final question that allows for the respondent to say whatever it is they have been dying to tell you but you’ve forgotten to ask. About half the time they are tired too and will tell you they have nothing else to say. But incredibly, some of the most honest and complete responses take place here, at the end of a long interview. You have to realize that the person being interviewed is often discovering things about themselves as they talk to you and that this process of discovery can lead to new insights for them. Making space at the end is therefore crucial. Be sure you convey that you actually do want them to tell you more, that the offer of “anything else?” is not read as an empty convention where the polite response is no. Here is where you can pull from that active listening and tailor the final question to the particular person. For example, “I’ve asked you a lot of questions about what it was like to live through that wildfire. I’m wondering if there is anything I’ve forgotten to ask, especially because I haven’t had that experience myself” is a much more inviting final question than “Great. Anything you want to add?” It’s also helpful to convey to the person that you have the time to listen to their full answer, even if the allotted time is at the end. After all, there are no more questions to ask, so the respondent knows exactly how much time is left. Do them the courtesy of listening to them!
Conducting the Interview
Once you have your interview guide, you are on your way to conducting your first interview. I always practice my interview guide with a friend or family member. I do this even when the questions don’t make perfect sense for them, as it still helps me realize which questions make no sense, are poorly worded (too academic), or don’t follow sequentially. I also practice the routine I will use for interviewing, which goes something like this:
- Introduce myself and reintroduce the study
- Provide consent form and ask them to sign and retain/return copy
- Ask if they have any questions about the study before we begin
- Ask if I can begin recording
- Ask questions (from interview guide)
- Turn off the recording device
- Ask if they are willing to fill out my demographic questionnaire
- Collect questionnaire and, without looking at the answers, place in same folder as signed consent form
- Thank them and depart
A note on remote interviewing: Interviews have traditionally been conducted face-to-face in a private or quiet public setting. You don’t want a lot of background noise, as this will make transcriptions difficult. During the recent global pandemic, many interviewers, myself included, learned the benefits of interviewing remotely. Although face-to-face is still preferable for many reasons, Zoom interviewing is not a bad alternative, and it does allow more interviews across great distances. Zoom also includes automatic transcription, which significantly cuts down on the time it normally takes to convert our conversations into “data” to be analyzed. These automatic transcriptions are not perfect, however, and you will still need to listen to the recording and clarify and clean up the transcription. Nor do automatic transcriptions include notations of body language or change of tone, which you may want to include. When interviewing remotely, you will want to collect the consent form before you meet: ask them to read, sign, and return it as an email attachment. I think it is better to ask for the demographic questionnaire after the interview, but because some respondents may never return it then, it is probably best to ask for this at the same time as the consent form, in advance of the interview.
What should you bring to the interview? I would recommend bringing two copies of the consent form (one for you and one for the respondent), a demographic questionnaire, a manila folder in which to place the signed consent form and filled-out demographic questionnaire, a printed copy of your interview guide (I print with three-inch right margins so I can jot down notes on the page next to relevant questions), a pen, a recording device, and water.
After the interview, you will want to secure the signed consent form in a locked filing cabinet (if in print) or a password-protected folder on your computer. Using Excel or a similar program that allows tables/spreadsheets, create an identifying number for your interview that links to the consent form without using the name of your respondent. For example, let’s say that I conduct interviews with US politicians, and the first person I meet with is George W. Bush. I will assign the transcription the number “INT#001” and add it to the signed consent form. [3] The signed consent form goes into a locked filing cabinet, and I never use the name “George W. Bush” again. I take the information from the demographic sheet, open my Excel spreadsheet, and add the relevant information in separate columns for the row INT#001: White, male, Republican. When I interview Bill Clinton as my second interview, I include a second row: INT#002: White, male, Democrat. And so on. The only link to the actual name of the respondent and this information is the fact that the consent form (unavailable to anyone but me) has stamped on it the interview number.
Many students get very nervous before their first interview. Actually, many of us are always nervous before the interview! But do not worry—this is normal, and it does pass. Chances are, you will be pleasantly surprised at how comfortable it begins to feel. These “purposeful conversations” are often a delight for both participants. This is not to say that sometimes things go wrong. I often have my students practice several “bad scenarios” (e.g., a respondent that you cannot get to open up; a respondent who is too talkative and dominates the conversation, steering it away from the topics you are interested in; emotions that completely take over; or shocking disclosures you are ill-prepared to handle), but most of the time, things go quite well. Be prepared for the unexpected, but know that the reason interviews are so popular as a technique of data collection is that they are usually richly rewarding for both participants.
One thing that I stress to my methods students and remind myself about is that interviews are still conversations between people. If there’s something you might feel uncomfortable asking someone about in a “normal” conversation, you will likely also feel a bit of discomfort asking it in an interview. Maybe more importantly, your respondent may feel uncomfortable. Social research—especially about inequality—can be uncomfortable. And it’s easy to slip into an abstract, intellectualized, or removed perspective as an interviewer. This is one reason trying out interview questions is important. Another is that sometimes the question sounds good in your head but doesn’t work as well out loud in practice. I learned this the hard way when a respondent asked me how I would answer the question I had just posed, and I realized that not only did I not really know how I would answer it, but I also wasn’t quite as sure I knew what I was asking as I had thought.
—Elizabeth M. Lee, Associate Professor of Sociology at Saint Joseph’s University, author of Class and Campus Life , and co-author of Geographies of Campus Inequality
How Many Interviews?
Your research design has included a targeted number of interviews and a recruitment plan (see chapter 5). Follow your plan, but remember that “ saturation ” is your goal. You interview as many people as you can until you reach a point at which you are no longer surprised by what they tell you. This means not that no one after your first twenty interviews will have surprising, interesting stories to tell you but rather that the picture you are forming about the phenomenon of interest to you from a research perspective has come into focus, and none of the interviews are substantially refocusing that picture. That is when you should stop collecting interviews. Note that to know when you have reached this, you will need to read your transcripts as you go. More about this in chapters 18 and 19.
Your Final Product: The Ideal Interview Transcript
A good interview transcript will demonstrate a subtly controlled conversation by the skillful interviewer. In general, you want to see replies that are about one paragraph long, not short sentences and not running on for several pages. Although it is sometimes necessary to follow respondents down tangents, it is also often necessary to pull them back to the questions that form the basis of your research study. This is not really a free conversation, although it may feel like that to the person you are interviewing.
Final Tips from an Interview Master
Annette Lareau is arguably one of the masters of the trade. In Listening to People , she provides several guidelines for good interviews and then offers a detailed example of an interview gone wrong and how it could be addressed (please see the “Further Readings” at the end of this chapter). Here is an abbreviated version of her set of guidelines: (1) interview respondents who are experts on the subjects of most interest to you (as a corollary, don’t ask people about things they don’t know); (2) listen carefully and talk as little as possible; (3) keep in mind what you want to know and why you want to know it; (4) be a proactive interviewer (subtly guide the conversation); (5) assure respondents that there aren’t any right or wrong answers; (6) use the respondent’s own words to probe further (this both allows you to accurately identify what you heard and pushes the respondent to explain further); (7) reuse effective probes (don’t reinvent the wheel as you go—if repeating the words back works, do it again and again); (8) focus on learning the subjective meanings that events or experiences have for a respondent; (9) don’t be afraid to ask a question that draws on your own knowledge (unlike trial lawyers who are trained never to ask a question for which they don’t already know the answer, sometimes it’s worth it to ask risky questions based on your hypotheses or just plain hunches); (10) keep thinking while you are listening (so difficult…and important); (11) return to a theme raised by a respondent if you want further information; (12) be mindful of power inequalities (and never ever coerce a respondent to continue the interview if they want out); (13) take control with overly talkative respondents; (14) expect overly succinct responses, and develop strategies for probing further; (15) balance digging deep and moving on; (16) develop a plan to deflect questions (e.g., let them know you are happy to answer any questions at the end of the interview, but you don’t want to take time away from them now); and at the end, (17) check to see whether you have asked all your questions. You don’t always have to ask everyone the same set of questions, but if there is a big area you have forgotten to cover, now is the time to recover ( Lareau 2021:93–103 ).
Sample: Demographic Questionnaire
ASA Taskforce on First-Generation and Working-Class Persons in Sociology – Class Effects on Career Success
Supplementary Demographic Questionnaire
Thank you for your participation in this interview project. We would like to collect a few pieces of key demographic information from you to supplement our analyses. Your answers to these questions will be kept confidential and stored by ID number. All of your responses here are entirely voluntary!
What best captures your race/ethnicity? (please check any/all that apply)
- White (Non Hispanic/Latina/o/x)
- Black or African American
- Hispanic, Latino/a/x of Spanish
- Asian or Asian American
- American Indian or Alaska Native
- Middle Eastern or North African
- Native Hawaiian or Pacific Islander
- Other : (Please write in: ________________)
What is your current position?
- Grad Student
- Full Professor
Please check any and all of the following that apply to you:
- I identify as a working-class academic
- I was the first in my family to graduate from college
- I grew up poor
What best reflects your gender?
- Transgender female/Transgender woman
- Transgender male/Transgender man
- Gender queer/ Gender nonconforming
Anything else you would like us to know about you?
Example: Interview Guide
In this example, follow-up prompts are italicized. Note the sequence of questions. That second question often elicits an entire life history , answering several later questions in advance.
Introduction Script/Question
Thank you for participating in our survey of ASA members who identify as first-generation or working-class. As you may have heard, ASA has sponsored a taskforce on first-generation and working-class persons in sociology and we are interested in hearing from those who so identify. Your participation in this interview will help advance our knowledge in this area.
- The first thing we would like to as you is why you have volunteered to be part of this study? What does it mean to you be first-gen or working class? Why were you willing to be interviewed?
- How did you decide to become a sociologist?
- Can you tell me a little bit about where you grew up? ( prompts: what did your parent(s) do for a living? What kind of high school did you attend?)
- Has this identity been salient to your experience? (how? How much?)
- How welcoming was your grad program? Your first academic employer?
- Why did you decide to pursue sociology at the graduate level?
- Did you experience culture shock in college? In graduate school?
- Has your FGWC status shaped how you’ve thought about where you went to school? debt? etc?
- Were you mentored? How did this work (not work)? How might it?
- What did you consider when deciding where to go to grad school? Where to apply for your first position?
- What, to you, is a mark of career success? Have you achieved that success? What has helped or hindered your pursuit of success?
- Do you think sociology, as a field, cares about prestige?
- Let’s talk a little bit about intersectionality. How does being first-gen/working class work alongside other identities that are important to you?
- What do your friends and family think about your career? Have you had any difficulty relating to family members or past friends since becoming highly educated?
- Do you have any debt from college/grad school? Are you concerned about this? Could you explain more about how you paid for college/grad school? (here, include assistance from family, fellowships, scholarships, etc.)
- (You’ve mentioned issues or obstacles you had because of your background.) What could have helped? Or, who or what did? Can you think of fortuitous moments in your career?
- Do you have any regrets about the path you took?
- Is there anything else you would like to add? Anything that the Taskforce should take note of, that we did not ask you about here?
Further Readings
Britten, Nicky. 1995. “Qualitative Interviews in Medical Research.” BMJ: British Medical Journal 31(6999):251–253. A good basic overview of interviewing particularly useful for students of public health and medical research generally.
Corbin, Juliet, and Janice M. Morse. 2003. “The Unstructured Interactive Interview: Issues of Reciprocity and Risks When Dealing with Sensitive Topics.” Qualitative Inquiry 9(3):335–354. Weighs the potential benefits and harms of conducting interviews on topics that may cause emotional distress. Argues that the researcher’s skills and code of ethics should ensure that the interviewing process provides more of a benefit to both participant and researcher than a harm to the former.
Gerson, Kathleen, and Sarah Damaske. 2020. The Science and Art of Interviewing . New York: Oxford University Press. A useful guidebook/textbook for both undergraduates and graduate students, written by sociologists.
Kvale, Steiner. 2007. Doing Interviews . London: SAGE. An easy-to-follow guide to conducting and analyzing interviews by psychologists.
Lamont, Michèle, and Ann Swidler. 2014. “Methodological Pluralism and the Possibilities and Limits of Interviewing.” Qualitative Sociology 37(2):153–171. Written as a response to various debates surrounding the relative value of interview-based studies and ethnographic studies defending the particular strengths of interviewing. This is a must-read article for anyone seriously engaging in qualitative research!
Pugh, Allison J. 2013. “What Good Are Interviews for Thinking about Culture? Demystifying Interpretive Analysis.” American Journal of Cultural Sociology 1(1):42–68. Another defense of interviewing written against those who champion ethnographic methods as superior, particularly in the area of studying culture. A classic.
Rapley, Timothy John. 2001. “The ‘Artfulness’ of Open-Ended Interviewing: Some considerations in analyzing interviews.” Qualitative Research 1(3):303–323. Argues for the importance of “local context” of data production (the relationship built between interviewer and interviewee, for example) in properly analyzing interview data.
Weiss, Robert S. 1995. Learning from Strangers: The Art and Method of Qualitative Interview Studies . New York: Simon and Schuster. A classic and well-regarded textbook on interviewing. Because Weiss has extensive experience conducting surveys, he contrasts the qualitative interview with the survey questionnaire well; particularly useful for those trained in the latter.
- I say “normally” because how people understand their various identities can itself be an expansive topic of inquiry. Here, I am merely talking about collecting otherwise unexamined demographic data, similar to how we ask people to check boxes on surveys. ↵
- Again, this applies to “semistructured in-depth interviewing.” When conducting standardized questionnaires, you will want to ask each question exactly as written, without deviations! ↵
- I always include “INT” in the number because I sometimes have other kinds of data with their own numbering: FG#001 would mean the first focus group, for example. I also always include three-digit spaces, as this allows for up to 999 interviews (or, more realistically, allows for me to interview up to one hundred persons without having to reset my numbering system). ↵
A method of data collection in which the researcher asks the participant questions; the answers to these questions are often recorded and transcribed verbatim. There are many different kinds of interviews - see also semistructured interview , structured interview , and unstructured interview .
A document listing key questions and question areas for use during an interview. It is used most often for semi-structured interviews. A good interview guide may have no more than ten primary questions for two hours of interviewing, but these ten questions will be supplemented by probes and relevant follow-ups throughout the interview. Most IRBs require the inclusion of the interview guide in applications for review. See also interview and semi-structured interview .
A data-collection method that relies on casual, conversational, and informal interviewing. Despite its apparent conversational nature, the researcher usually has a set of particular questions or question areas in mind but allows the interview to unfold spontaneously. This is a common data-collection technique among ethnographers. Compare to the semi-structured or in-depth interview .
A form of interview that follows a standard guide of questions asked, although the order of the questions may change to match the particular needs of each individual interview subject, and probing “follow-up” questions are often added during the course of the interview. The semi-structured interview is the primary form of interviewing used by qualitative researchers in the social sciences. It is sometimes referred to as an “in-depth” interview. See also interview and interview guide .
The cluster of data-collection tools and techniques that involve observing interactions between people, the behaviors, and practices of individuals (sometimes in contrast to what they say about how they act and behave), and cultures in context. Observational methods are the key tools employed by ethnographers and Grounded Theory .
Follow-up questions used in a semi-structured interview to elicit further elaboration. Suggested prompts can be included in the interview guide to be used/deployed depending on how the initial question was answered or if the topic of the prompt does not emerge spontaneously.
A form of interview that follows a strict set of questions, asked in a particular order, for all interview subjects. The questions are also the kind that elicits short answers, and the data is more “informative” than probing. This is often used in mixed-methods studies, accompanying a survey instrument. Because there is no room for nuance or the exploration of meaning in structured interviews, qualitative researchers tend to employ semi-structured interviews instead. See also interview.
The point at which you can conclude data collection because every person you are interviewing, the interaction you are observing, or content you are analyzing merely confirms what you have already noted. Achieving saturation is often used as the justification for the final sample size.
An interview variant in which a person’s life story is elicited in a narrative form. Turning points and key themes are established by the researcher and used as data points for further analysis.
Introduction to Qualitative Research Methods Copyright © 2023 by Allison Hurst is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License , except where otherwise noted.
Have a language expert improve your writing
Run a free plagiarism check in 10 minutes, automatically generate references for free.
- Knowledge Base
- Methodology
- Types of Interviews in Research | Guide & Examples
Types of Interviews in Research | Guide & Examples
Published on 4 May 2022 by Tegan George . Revised on 10 October 2022.
An interview is a qualitative research method that relies on asking questions in order to collect data . Interviews involve two or more people, one of whom is the interviewer asking the questions.
There are several types of interviews, often differentiated by their level of structure. Structured interviews have predetermined questions asked in a predetermined order. Unstructured interviews are more free-flowing, and semi-structured interviews fall in between.
Interviews are commonly used in market research, social science, and ethnographic research.
Table of contents
What is a structured interview, what is a semi-structured interview, what is an unstructured interview, what is a focus group, examples of interview questions, advantages and disadvantages of interviews, frequently asked questions about types of interviews.
Structured interviews have predetermined questions in a set order. They are often closed-ended, featuring dichotomous (yes/no) or multiple-choice questions. While open-ended structured interviews exist, they are much less common. The types of questions asked make structured interviews a predominantly quantitative tool.
Asking set questions in a set order can help you see patterns among responses, and it allows you to easily compare responses between participants while keeping other factors constant. This can mitigate biases and lead to higher reliability and validity. However, structured interviews can be overly formal, as well as limited in scope and flexibility.
- You feel very comfortable with your topic. This will help you formulate your questions most effectively.
- You have limited time or resources. Structured interviews are a bit more straightforward to analyse because of their closed-ended nature, and can be a doable undertaking for an individual.
- Your research question depends on holding environmental conditions between participants constant
Prevent plagiarism, run a free check.
Semi-structured interviews are a blend of structured and unstructured interviews. While the interviewer has a general plan for what they want to ask, the questions do not have to follow a particular phrasing or order.
Semi-structured interviews are often open-ended, allowing for flexibility, but follow a predetermined thematic framework, giving a sense of order. For this reason, they are often considered ‘the best of both worlds’.
However, if the questions differ substantially between participants, it can be challenging to look for patterns, lessening the generalisability and validity of your results.
- You have prior interview experience. It’s easier than you think to accidentally ask a leading question when coming up with questions on the fly. Overall, spontaneous questions are much more difficult than they may seem.
- Your research question is exploratory in nature. The answers you receive can help guide your future research.
An unstructured interview is the most flexible type of interview. The questions and the order in which they are asked are not set. Instead, the interview can proceed more spontaneously, based on the participant’s previous answers.
Unstructured interviews are by definition open-ended. This flexibility can help you gather detailed information on your topic, while still allowing you to observe patterns between participants.
However, so much flexibility means that they can be very challenging to conduct properly. You must be very careful not to ask leading questions, as biased responses can lead to lower reliability or even invalidate your research.
- You have a solid background in your research topic and have conducted interviews before
- Your research question is exploratory in nature, and you are seeking descriptive data that will deepen and contextualise your initial hypotheses
- Your research necessitates forming a deeper connection with your participants, encouraging them to feel comfortable revealing their true opinions and emotions
A focus group brings together a group of participants to answer questions on a topic of interest in a moderated setting. Focus groups are qualitative in nature and often study the group’s dynamic and body language in addition to their answers. Responses can guide future research on consumer products and services, human behaviour, or controversial topics.
Focus groups can provide more nuanced and unfiltered feedback than individual interviews and are easier to organise than experiments or large surveys. However, their small size leads to low external validity and the temptation as a researcher to ‘cherry-pick’ responses that fit your hypotheses.
- Your research focuses on the dynamics of group discussion or real-time responses to your topic
- Your questions are complex and rooted in feelings, opinions, and perceptions that cannot be answered with a ‘yes’ or ‘no’
- Your topic is exploratory in nature, and you are seeking information that will help you uncover new questions or future research ideas
Depending on the type of interview you are conducting, your questions will differ in style, phrasing, and intention. Structured interview questions are set and precise, while the other types of interviews allow for more open-endedness and flexibility.
Here are some examples.
- Semi-structured
- Unstructured
- Focus group
- Do you like dogs? Yes/No
- Do you associate dogs with feeling: happy; somewhat happy; neutral; somewhat unhappy; unhappy
- If yes, name one attribute of dogs that you like.
- If no, name one attribute of dogs that you don’t like.
- What feelings do dogs bring out in you?
- When you think more deeply about this, what experiences would you say your feelings are rooted in?
Interviews are a great research tool. They allow you to gather rich information and draw more detailed conclusions than other research methods, taking into consideration nonverbal cues, off-the-cuff reactions, and emotional responses.
However, they can also be time-consuming and deceptively challenging to conduct properly. Smaller sample sizes can cause their validity and reliability to suffer, and there is an inherent risk of interviewer effect arising from accidentally leading questions.
Here are some advantages and disadvantages of each type of interview that can help you decide if you’d like to utilise this research method.
| Type of interview | Advantages | Disadvantages |
|---|---|---|
| Structured interview | ||
| Semi-structured interview | ||
| Unstructured interview | ||
| Focus group |
The four most common types of interviews are:
- Structured interviews : The questions are predetermined in both topic and order.
- Semi-structured interviews : A few questions are predetermined, but other questions aren’t planned.
- Unstructured interviews : None of the questions are predetermined.
- Focus group interviews : The questions are presented to a group instead of one individual.
A structured interview is a data collection method that relies on asking questions in a set order to collect data on a topic. They are often quantitative in nature. Structured interviews are best used when:
- You already have a very clear understanding of your topic. Perhaps significant research has already been conducted, or you have done some prior research yourself, but you already possess a baseline for designing strong structured questions.
- You are constrained in terms of time or resources and need to analyse your data quickly and efficiently
- Your research question depends on strong parity between participants, with environmental conditions held constant
More flexible interview options include semi-structured interviews , unstructured interviews , and focus groups .
A semi-structured interview is a blend of structured and unstructured types of interviews. Semi-structured interviews are best used when:
- You have prior interview experience. Spontaneous questions are deceptively challenging, and it’s easy to accidentally ask a leading question or make a participant uncomfortable.
- Your research question is exploratory in nature. Participant answers can guide future research questions and help you develop a more robust knowledge base for future research.
An unstructured interview is the most flexible type of interview, but it is not always the best fit for your research topic.
Unstructured interviews are best used when:
- You are an experienced interviewer and have a very strong background in your research topic, since it is challenging to ask spontaneous, colloquial questions
- Your research question is exploratory in nature. While you may have developed hypotheses, you are open to discovering new or shifting viewpoints through the interview process.
- You are seeking descriptive data, and are ready to ask questions that will deepen and contextualise your initial thoughts and hypotheses
- Your research depends on forming connections with your participants and making them feel comfortable revealing deeper emotions, lived experiences, or thoughts
The interviewer effect is a type of bias that emerges when a characteristic of an interviewer (race, age, gender identity, etc.) influences the responses given by the interviewee.
There is a risk of an interviewer effect in all types of interviews , but it can be mitigated by writing really high-quality interview questions.
Cite this Scribbr article
If you want to cite this source, you can copy and paste the citation or click the ‘Cite this Scribbr article’ button to automatically add the citation to our free Reference Generator.
George, T. (2022, October 10). Types of Interviews in Research | Guide & Examples. Scribbr. Retrieved 3 September 2024, from https://www.scribbr.co.uk/research-methods/types-of-interviews/
Is this article helpful?

Tegan George
Other students also liked, data collection methods | step-by-step guide & examples, face validity | guide with definition & examples, construct validity | definition, types, & examples.

3 Types of Interviews in Qualitative Research: An Essential Research Instrument and Handy Tips to Conduct Them
Introduction.
Qualitative research is one of the research methodologies used in various fields to gain a deeper understanding of complex phenomena. It involves exploring and interpreting subjective experiences, beliefs, and behaviors of individuals or groups.
One of the key tools used in qualitative research is interviews which allow researchers to gather rich and detailed data directly from participants. In this comprehensive guide, we will delve into the use of interviews as one of the primary data collection method in qualitative research. We will explore the significance of interviews, different approaches to conducting interviews, and the steps involved in preparing for and conducting successful interviews. Additionally, we will discuss the process of analyzing and interpreting interview data, as well as presenting research findings.

If you are a student starting a research project or a seasoned researcher aiming to enhance your qualitative research skills, this guide will equip you with the necessary knowledge and strategies to master the use of interviews in qualitative research. By the end of this guide, you will have a solid understanding of how to effectively utilize interviews to gather valuable insights and contribute to the body of qualitative research.
An Overview of Qualitative Research
Qualitative research is a method of inquiry that aims to understand and interpret social phenomena. It involves collecting and analyzing non-numerical data to gain insights into concepts, opinions, or experiences. Unlike quantitative research, which focuses on numerical data and statistical analysis, qualitative research emphasizes the exploration of meanings, perspectives, and context. In qualitative research, the researcher seeks to understand the subjective experiences and perspectives of individuals or groups. This approach allows for a deeper understanding of complex social phenomena that cannot be easily quantified. Qualitative research methods include interviews, observations, and analysis of documents or artifacts.
The Significance of Interviews in Qualitative Research
Interviews play a crucial role in qualitative research as they provide researchers with a unique opportunity to gather rich and detailed data directly from participants.
Exploring Subjective Experiences Through Interviews
One of the main reasons why interviews are significant in qualitative research is that they allow researchers to explore the subjective experiences, perspectives, and meanings that individuals attach to a particular phenomenon. Through interviews, researchers can delve deep into the thoughts, emotions, and motivations of participants, gaining a comprehensive understanding of their lived experiences.
Capturing Nuances and Building Rapport
Moreover, interviews enable researchers to capture the nuances and complexities of human behavior and social interactions, which may not be easily observable through other research methods. By engaging in face-to-face or virtual conversations with participants, researchers can establish rapport and trust, creating a comfortable environment for participants to share their thoughts and experiences openly. This personal interaction fosters a deeper level of engagement and allows researchers to ask follow-up questions, probe for more detailed responses, and clarify any ambiguities. Additionally, interviews provide researchers with the flexibility to adapt their questioning techniques and explore emerging themes or unexpected insights that may arise during the interview process.
Enhancing Research Credibility
The significance of interviews in qualitative research extends beyond data collection. Interviews also offer researchers the opportunity to validate and triangulate findings from other data sources. By comparing and contrasting the information obtained through interviews with data from observations, documents, or surveys, researchers can enhance the credibility and trustworthiness of their research findings.
Interviews are a common method used in qualitative research to gather data and gain insights into participants’ experiences, perspectives, and opinions. In an interview, researchers ask participants a series of open-ended questions, allowing them to provide detailed and in-depth responses. Interviews can be conducted in various formats, including face-to-face, phone, or online.
The main purpose of interviews is to collect rich and nuanced data that cannot be easily obtained through other research methods. By engaging in direct conversations with participants, researchers can explore complex topics, probe for deeper understanding, and uncover new insights. Interviews also allow researchers to establish rapport with participants, creating a comfortable and trusting environment for open and honest discussions.
There are different types of interviews that can be used in qualitative research, including structured interviews, semi-structured interviews, and unstructured interviews. Each type of interview has its own advantages and is suitable for different research objectives and contexts.
Structured Interviews
What is Structured Interviews?
Structured interviews are a type of qualitative research instrument that follows a predetermined set of questions in a specific order. This method is commonly used in social sciences and market research to collect data on a particular topic. The main characteristic of structured interviews is that the questions are standardized and asked in the same way to all participants. This ensures consistency and allows for easy comparison of responses. The questions are carefully designed to elicit specific answers that align with the objectives of the study.
Structured interviews are often conducted face-to-face or through telephone or online platforms. The interviewer follows a script or questionnaire that outlines the procedure of the interview. This script includes the exact wording of the questions and any prompts or probes that may be used to clarify or expand on the participant’s responses.
Advantages of Structured Interviews
One advantage of structured interviews is that they provide a high level of control over the data collection process. The standardized nature of the questions allows for reliable and replicable data. Additionally, structured interviews are efficient as they can be administered to multiple participants in a relatively short period of time.
Limitations of Structured Interviews
However, structured interviews also have some limitations. The predetermined set of questions may restrict participants from fully expressing their thoughts or experiences. This can limit the depth of information obtained. Moreover, structured interviews may not be suitable for exploring complex or sensitive topics that require more flexibility and open-ended responses.
Semi-Structured Interviews
What is Semi-Structured Interviews?
Semi-structured interviews are a commonly used qualitative research instrument that combines the flexibility of open-ended questions with the structure of predetermined themes or topics. In a semi-structured interview, the researcher prepares a set of open-ended questions that are designed to explore specific areas of interest. These questions serve as a guide for the interview, but the interviewer has the flexibility to ask follow-up questions or probe deeper into certain topics based on the participant’s responses. The use of semi-structured interviews allows for a more nuanced understanding of the research topic . It allows participants to express their thoughts and experiences in their own words, providing rich and detailed data.
Advantages of Semi-Structured Interviews
One of the advantages of semi-structured interviews is that they can be adapted to different research contexts and participant characteristics. The researcher can tailor the interview questions to suit the specific needs of the study and the participants involved.
Another advantage of semi-structured interviews is that they allow for the exploration of unexpected or emergent themes. As the interview progresses, new ideas or perspectives may arise, and the interviewer can delve deeper into these areas to gain a deeper understanding of the research topic.
Limitations of Semi-Structured Interviews
However, conducting semi-structured interviews requires skill and experience on the part of the researcher. The interviewer must be able to create a comfortable and non-threatening environment for the participant, as well as actively listen and engage in the conversation. In addition, the analysis of semi-structured interview data can be time-consuming and complex. The researcher must carefully transcribe and code the interview recordings, and then analyze the data to identify patterns, themes, and insights.
Unstructured Interviews
What is Unstructured Interviews?
Unstructured interviews are a popular research tool used by teams looking to take an exploratory and open approach to collect information about a topic. As the name suggests, unstructured interviews are among the least predictable and most dynamic methods of qualitative research. They rely on asking participants questions to collect data on a topic without a predetermined set of questions or a strict interview guide.
The unstructured interview technique was developed to allow researchers to delve deeper into the thoughts, experiences, and perspectives of participants. It provides a flexible and fluid conversation that allows for the emergence of new insights and unexpected findings. Unlike structured interviews, unstructured interviews do not follow a specific format or set of questions. Instead, the interviewer relies on prompts or probes to remind them about topics to discuss.
Advantages of Unstructured Interviews
Unstructured interviews offer several advantages in qualitative research. They allow for a more natural and conversational interaction between the interviewer and the participant, creating a comfortable environment for the participant to share their thoughts and experiences. This can lead to rich and detailed data that provides a deeper understanding of the research topic. Additionally, unstructured interviews provide the flexibility to explore new avenues of inquiry and follow-up on interesting responses, allowing for the discovery of unexpected insights.
Limitations of Unstructured Interviews
However, unstructured interviews also have some limitations. The lack of a predetermined set of questions can make it challenging to compare and analyze data across participants. The open-ended nature of the interviews can also result in a large amount of data that needs to be carefully analyzed. Furthermore, the interviewer’s skills and biases can influence the direction and depth of the conversation, potentially impacting the validity and reliability of the findings.
Preparation for Successful Interviews in Research
Preparing for interviews in qualitative research is a crucial step that can greatly impact the quality of data collected. By taking the time to adequately prepare, researchers can ensure that they are asking the right questions and gathering the necessary information to answer their research questions .
Clearly Defining Research Objectives
The first step in preparing for interviews is to clearly define the research objectives and the specific information that needs to be collected. This involves identifying the key research questions and outlining the broad areas of knowledge that are relevant to answering these questions. By doing so, researchers can focus their interviews on gathering the most relevant and valuable data.
Developing a Detailed Interview Guide
Once the research objectives are defined, the next step is to develop a detailed interview guide or protocol. This guide serves as a roadmap for the interview and helps ensure that all necessary topics are covered. The guide should include a list of questions or prompts that will be used during the interview, as well as any follow-up questions that may be necessary. It is important to strike a balance between having a structured guide and allowing for flexibility to explore unexpected insights.
Conducting Preliminary Research
In addition to developing the interview guide, researchers should also conduct preliminary research on the topic and the interviewee. This includes familiarizing themselves with the existing literature and theories related to the research topic, as well as gaining an understanding of the interviewee’s background and expertise. This background knowledge will not only help researchers ask informed and relevant questions but also establish a rapport with the interviewee.
Practicing the Interview Process
Another important aspect of preparation is practicing the interview. Researchers should take the time to rehearse the interview process, either by conducting mock interviews with colleagues or by recording and reviewing their own interviews. This practice allows researchers to refine their questioning techniques, identify any potential issues or biases, and ensure that the interview flows smoothly.
Creating a Conducive Environment
Lastly, it is crucial to establish a comfortable and conducive environment for the interview. This includes selecting a quiet and private location where both the interviewer and interviewee can focus without distractions. It is also important to ensure that any necessary equipment, such as recording devices or note-taking materials, are prepared and functioning properly.
Handy Tips for Conducting Effective Interviews
1. Establish rapport: Building a rapport with the interviewee is crucial for creating a comfortable and open environment. Begin the interview by introducing yourself and explaining the purpose of the interview. Show genuine interest in the interviewee’s perspective and make them feel valued.
2. Use active listening: Active listening is a key skill in conducting effective interviews. Pay close attention to the interviewee’s responses, maintain eye contact, and nod or provide verbal cues to show that you are engaged. Avoid interrupting and allow the interviewee to fully express their thoughts.
3. Ask open-ended questions: Open-ended questions encourage the interviewee to provide detailed and thoughtful responses. Instead of asking yes or no questions, ask questions that begin with words like ‘how,’ ‘why,’ or ‘tell me about.’ This allows the interviewee to share their experiences, opinions, and insights.
4. Follow-up with probing questions: Probing questions help to delve deeper into a particular topic or clarify ambiguous responses. These questions can be used to gather more specific information or to explore different perspectives. Examples of probing questions include ‘Can you provide an example?’ or ‘Could you elaborate on that?’
5. Maintain a neutral stance: It is important for the interviewer to remain neutral and unbiased throughout the interview. Avoid expressing personal opinions or judgments that may influence the interviewee’s responses. This allows for a more objective and authentic data collection process.
6. Adapt to the interviewee’s communication style: People have different communication styles, and it is essential to adapt to the interviewee’s preferred style. Some individuals may prefer a more formal and structured approach, while others may respond better to a conversational and relaxed style. Pay attention to verbal and non-verbal cues to gauge the interviewee’s comfort level.
7. Record and document the interview: To ensure accuracy and avoid missing important details, it is recommended to record the interview with the interviewee’s consent. This allows for a thorough analysis of the data and provides a reference for future reference. Take detailed notes during the interview to capture key points and observations.
8. Respect confidentiality and ethical considerations: Interviews often involve sensitive and personal information. It is crucial to respect the interviewee’s confidentiality and privacy. Obtain informed consent and assure the interviewee that their responses will be kept confidential. Adhere to ethical guidelines and ensure the data is used responsibly and ethically.
9. Reflect on the interview process: After conducting the interview, take time to reflect on the process. Evaluate the effectiveness of your questions, the flow of the conversation, and any challenges encountered. Reflecting on the interview allows for continuous improvement and enhances the quality of future interviews.
By following these guidelines, researchers can conduct effective interviews that yield rich and valuable qualitative data. Effective interviews contribute to the depth and quality of the research findings, providing valuable insights into the research topic.
Methods for Analyzing and Interpreting the Interview Data
Once the interviews have been conducted and recorded, the next step in qualitative research is to analyze and interpret the interview data. This process involves carefully examining the transcripts or recordings of the interviews to identify patterns, themes, and insights.
Transcribing the Interview Datas
One common method for analyzing interview data is through transcription. Transcription involves transcribing the interviews word-for-word, capturing every detail and nuance of the conversation. This allows researchers to closely examine the content of the interviews and identify key themes and ideas.
Applying Thematic Analysis
After transcribing the interviews, researchers can use various techniques to analyze the data. One approach is thematic analysis, which involves identifying recurring themes or patterns in the interview data. Researchers can use coding software or manual techniques to identify and categorize these themes, allowing for a deeper understanding of the data.
Interpreting Research Findings
Once the data has been analyzed and coded, researchers can begin interpreting the findings. This involves making sense of the data and drawing conclusions based on the patterns and themes that have emerged. Researchers may also compare the findings to existing theories or literature to provide further context and insight.
Maintaining Transparency and Rigor
It is important to note that analyzing and interpreting interview data is a subjective process. Researchers bring their own perspectives and biases to the analysis, which can influence the interpretation of the data. Therefore, it is crucial to maintain transparency and rigor in the analysis process, documenting the steps taken and the decisions made.
Presenting Research Findings
Once you have completed the analysis and interpretation of your interview data, the next step is to present your research findings. This section will guide you on how to effectively present your qualitative research findings.
Presenting Data using Table
One common way to present interview data is by using a table. A table can help organize and summarize the key findings from your interviews. You can include information such as participant demographics, interview questions, and the main themes or categories that emerged from the data.
Using Quotes or Excerpts
In addition to tables, you can also use quotes or excerpts from the interviews to support your findings. Including direct quotes can add credibility to your research and provide a more in-depth understanding of the participants’ perspectives.
Providing a Clear and Concise Presentation of Research Findings
When presenting your findings, it is important to provide a clear and concise description of the main themes or patterns that emerged from the data. You should also discuss any unexpected or contradictory findings and provide possible explanations or interpretations.
Tailoring the Presentation According to the Audiences
Furthermore, it is crucial to consider the audience for your research findings. Depending on the intended audience, you may need to adapt your presentation style and language. For academic audiences, you may need to provide more detailed explanations and references to existing literature. For non-academic audiences, you may need to use simpler language and provide more practical implications of your findings.
Flexibility in Presenting Qualitative Research
Lastly, it is important to remember that presenting qualitative research findings is not a one-size-fits-all approach. The presentation format and style may vary depending on the nature of your research and the preferences of your audience. Therefore, it is essential to carefully consider the most appropriate way to present your findings to effectively communicate your research outcomes.
In short, interviews play a crucial role in qualitative research as they provide researchers with valuable insights and perspectives from participants. They allow researchers to delve deep into the experiences, beliefs, and motivations of individuals, providing rich and detailed data for analysis. By following the steps outlined in this guide, researchers can master the use of interviews and enhance the quality and validity of their qualitative research.
Leave a Comment Cancel reply
Save my name, email, and website in this browser for the next time I comment.
Related articles

How to Formulate Research Questions in a Research Proposal? Discover The No. 1 Easiest Template Here!

7 Easy Step-By-Step Guide of Using ChatGPT: The Best Literature Review Generator for Time-Saving Academic Research

Writing Engaging Introduction in Research Papers : 7 Tips and Tricks!

Understanding Comparative Frameworks: Their Importance, Components, Examples and 8 Best Practices

Revolutionizing Effective Thesis Writing for PhD Students Using Artificial Intelligence!

Highlight Abstracts: An Ultimate Guide For Researchers!

Crafting Critical Abstracts: 11 Expert Strategies for Summarizing Research

Crafting the Perfect Informative Abstract: Definition, Importance and 8 Expert Writing Tips
Qualitative Interviewing
- Reference work entry
- First Online: 13 January 2019
- Cite this reference work entry

- Sally Nathan 2 ,
- Christy Newman 3 &
- Kari Lancaster 3
4687 Accesses
26 Citations
8 Altmetric
Qualitative interviewing is a foundational method in qualitative research and is widely used in health research and the social sciences. Both qualitative semi-structured and in-depth unstructured interviews use verbal communication, mostly in face-to-face interactions, to collect data about the attitudes, beliefs, and experiences of participants. Interviews are an accessible, often affordable, and effective method to understand the socially situated world of research participants. The approach is typically informed by an interpretive framework where the data collected is not viewed as evidence of the truth or reality of a situation or experience but rather a context-bound subjective insight from the participants. The researcher needs to be open to new insights and to privilege the participant’s experience in data collection. The data from qualitative interviews is not generalizable, but its exploratory nature permits the collection of rich data which can answer questions about which little is already known. This chapter introduces the reader to qualitative interviewing, the range of traditions within which interviewing is utilized as a method, and highlights the advantages and some of the challenges and misconceptions in its application. The chapter also provides practical guidance on planning and conducting interview studies. Three case examples are presented to highlight the benefits and risks in the use of interviewing with different participants, providing situated insights as well as advice about how to go about learning to interview if you are a novice.
This is a preview of subscription content, log in via an institution to check access.
Access this chapter
Subscribe and save.
- Get 10 units per month
- Download Article/Chapter or eBook
- 1 Unit = 1 Article or 1 Chapter
- Cancel anytime
- Available as PDF
- Read on any device
- Instant download
- Own it forever
- Available as EPUB and PDF
- Durable hardcover edition
- Dispatched in 3 to 5 business days
- Free shipping worldwide - see info
Tax calculation will be finalised at checkout
Purchases are for personal use only
Institutional subscriptions
Similar content being viewed by others

Interviews in the social sciences

Interviewing in Qualitative Research
Baez B. Confidentiality in qualitative research: reflections on secrets, power and agency. Qual Res. 2002;2(1):35–58. https://doi.org/10.1177/1468794102002001638 .
Article Google Scholar
Braun V, Clarke V. Successful qualitative research: a practical guide for beginners. London: Sage Publications; 2013.
Google Scholar
Braun V, Clarke V, Gray D. Collecting qualitative data: a practical guide to textual, media and virtual techniques. Cambridge: Cambridge University Press; 2017.
Book Google Scholar
Bryman A. Social research methods. 5th ed. Oxford: Oxford University Press; 2016.
Crotty M. The foundations of social research: meaning and perspective in the research process. Australia: Allen & Unwin; 1998.
Davies MB. Doing a successful research project: using qualitative or quantitative methods. New York: Palgrave MacMillan; 2007.
Dickson-Swift V, James EL, Liamputtong P. Undertaking sensitive research in the health and social sciences. Cambridge: Cambridge University Press; 2008.
Foster M, Nathan S, Ferry M. The experience of drug-dependent adolescents in a therapeutic community. Drug Alcohol Rev. 2010;29(5):531–9.
Gillham B. The research interview. London: Continuum; 2000.
Glaser B, Strauss A. The discovery of grounded theory: strategies for qualitative research. Chicago: Aldine Publishing Company; 1967.
Hesse-Biber SN, Leavy P. In-depth interview. In: The practice of qualitative research. 2nd ed. Thousand Oaks: Sage Publications; 2011. p. 119–47
Irvine A. Duration, dominance and depth in telephone and face-to-face interviews: a comparative exploration. Int J Qual Methods. 2011;10(3):202–20.
Johnson JM. In-depth interviewing. In: Gubrium JF, Holstein JA, editors. Handbook of interview research: context and method. Thousand Oaks: Sage Publications; 2001.
Kvale S. Interviews: an introduction to qualitative research interviewing. Thousand Oaks: Sage; 1996.
Kvale S. Doing interviews. London: Sage Publications; 2007.
Lancaster K. Confidentiality, anonymity and power relations in elite interviewing: conducting qualitative policy research in a politicised domain. Int J Soc Res Methodol. 2017;20(1):93–103. https://doi.org/10.1080/13645579.2015.1123555 .
Leavy P. Method meets art: arts-based research practice. New York: Guilford Publications; 2015.
Liamputtong P. Researching the vulnerable: a guide to sensitive research methods. Thousand Oaks: Sage Publications; 2007.
Liamputtong P. Qualitative research methods. 4th ed. South Melbourne: Oxford University Press; 2013.
Mays N, Pope C. Quality in qualitative health research. In: Pope C, Mays N, editors. Qualitative research in health care. London: BMJ Books; 2000. p. 89–102.
McLellan E, MacQueen KM, Neidig JL. Beyond the qualitative interview: data preparation and transcription. Field Methods. 2003;15(1):63–84. https://doi.org/10.1177/1525822x02239573 .
Minichiello V, Aroni R, Hays T. In-depth interviewing: principles, techniques, analysis. 3rd ed. Sydney: Pearson Education Australia; 2008.
Morris ZS. The truth about interviewing elites. Politics. 2009;29(3):209–17. https://doi.org/10.1111/j.1467-9256.2009.01357.x .
Nathan S, Foster M, Ferry M. Peer and sexual relationships in the experience of drug-dependent adolescents in a therapeutic community. Drug Alcohol Rev. 2011;30(4):419–27.
National Health and Medical Research Council. National statement on ethical conduct in human research. Canberra: Australian Government; 2007.
Neal S, McLaughlin E. Researching up? Interviews, emotionality and policy-making elites. J Soc Policy. 2009;38(04):689–707. https://doi.org/10.1017/S0047279409990018 .
O’Reilly M, Parker N. ‘Unsatisfactory saturation’: a critical exploration of the notion of saturated sample sizes in qualitative research. Qual Res. 2013;13(2):190–7. https://doi.org/10.1177/1468794112446106 .
Ostrander S. “Surely you're not in this just to be helpful”: access, rapport and interviews in three studies of elites. In: Hertz R, Imber J, editors. Studying elites using qualitative methods. Thousand Oaks: Sage Publications; 1995. p. 133–50.
Chapter Google Scholar
Patton M. Qualitative research & evaluation methods: integrating theory and practice. Thousand Oaks: Sage Publications; 2015.
Punch KF. Introduction to social research: quantitative and qualitative approaches. London: Sage; 2005.
Rhodes T, Bernays S, Houmoller K. Parents who use drugs: accounting for damage and its limitation. Soc Sci Med. 2010;71(8):1489–97. https://doi.org/10.1016/j.socscimed.2010.07.028 .
Riessman CK. Narrative analysis. London: Sage; 1993.
Ritchie J. Not everything can be reduced to numbers. In: Berglund C, editor. Health research. Melbourne: Oxford University Press; 2001. p. 149–73.
Rubin H, Rubin I. Qualitative interviewing: the art of hearing data. 2nd ed. Thousand Oaks: Sage Publications; 2012.
Serry T, Liamputtong P. The in-depth interviewing method in health. In: Liamputtong P, editor. Research methods in health: foundations for evidence-based practice. 3rd ed. South Melbourne: Oxford University Press; 2017. p. 67–83.
Silverman D. Doing qualitative research. 5th ed. London: Sage; 2017.
Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (coreq): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–57. https://doi.org/10.1093/intqhc/mzm042 .
Download references
Author information
Authors and affiliations.
School of Public Health and Community Medicine, Faculty of Medicine, UNSW, Sydney, NSW, Australia
Sally Nathan
Centre for Social Research in Health, Faculty of Arts and Social Sciences, UNSW, Sydney, NSW, Australia
Christy Newman & Kari Lancaster
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to Sally Nathan .
Editor information
Editors and affiliations.
School of Science and Health, Western Sydney University, Penrith, NSW, Australia
Pranee Liamputtong
Rights and permissions
Reprints and permissions
Copyright information
© 2019 Springer Nature Singapore Pte Ltd.
About this entry
Cite this entry.
Nathan, S., Newman, C., Lancaster, K. (2019). Qualitative Interviewing. In: Liamputtong, P. (eds) Handbook of Research Methods in Health Social Sciences. Springer, Singapore. https://doi.org/10.1007/978-981-10-5251-4_77
Download citation
DOI : https://doi.org/10.1007/978-981-10-5251-4_77
Published : 13 January 2019
Publisher Name : Springer, Singapore
Print ISBN : 978-981-10-5250-7
Online ISBN : 978-981-10-5251-4
eBook Packages : Social Sciences Reference Module Humanities and Social Sciences Reference Module Business, Economics and Social Sciences
Share this entry
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Publish with us
Policies and ethics
- Find a journal
- Track your research
Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
Chapter 13: Interviews
Danielle Berkovic
Learning outcomes
Upon completion of this chapter, you should be able to:
- Understand when to use interviews in qualitative research.
- Develop interview questions for an interview guide.
- Understand how to conduct an interview.
What are interviews?
An interviewing method is the most commonly used data collection technique in qualitative research. 1 The purpose of an interview is to explore the experiences, understandings, opinions and motivations of research participants. 2 Interviews are conducted one-on-one with the researcher and the participant. Interviews are most appropriate when seeking to understand a participant’s subjective view of an experience and are also considered suitable for the exploration of sensitive topics.
What are the different types of interviews?
There are four main types of interviews:
- Key stakeholder: A key stakeholder interview aims to explore one issue in detail with a person of interest or importance concerning the research topic. 3 Key stakeholder interviews seek the views of experts on some cultural, political or health aspects of the community, beyond their personal beliefs or actions. An example of a key stakeholder is the Chief Health Officer of Victoria (Australia’s second-most populous state) who oversaw the world’s longest lockdowns in response to the COVID-19 pandemic.
- Dyad: A dyad interview aims to explore one issue in a level of detail with a dyad (two people). This form of interviewing is used when one participant of the dyad may need some support or is not wholly able to articulate themselves (e.g. people with cognitive impairment, or children). Independence is acknowledged and the interview is analysed as a unit. 4
- Narrative: A narrative interview helps individuals tell their stories, and prioritises their own perspectives and experiences using the language that they prefer. 5 This type of interview has been widely used in social research but is gaining prominence in health research to better understand person-centred care, for example, negotiating exercise and food abstinence whilst living with Type 2 diabetes. 6,7
- Life history: A life history interview allows the researcher to explore a person’s individual and subjective experiences within a history of the time framework. 8 Life history interviews challenge the researcher to understand how people’s current attitudes, behaviours and choices are influenced by previous experiences or trauma. Life history interviews have been conducted with Holocaust survivors 9 and youth who have been forcibly recruited to war. 10
Table 13.4 provides a summary of four studies, each adopting one of these types of interviews.
Interviewing techniques
There are two main interview techniques:
- Semi-structured: Semi-structured interviewing aims to explore a few issues in moderate detail, to expand the researcher’s knowledge at some level. 11 Semi-structured interviews give the researcher the advantage of remaining reasonably objective while enabling participants to share their perspectives and opinions. The researcher should create an interview guide with targeted open questions to direct the interview. As examples, semi-structured interviews have been used to extend knowledge of why women might gain excess weight during pregnancy, 12 and to update guidelines for statin uptake. 13
- In-depth: In-depth interviewing aims to explore a person’s subjective experiences and feelings about a particular topic. 14 In-depth interviews are often used to explore emotive (e.g. end-of-life care) 15 and complex (e.g. adolescent pregnancy) topics. 16 The researcher should create an interview guide with selected open questions to ask of the participant, but the participant should guide the direction of the interview more than in a semi-structured setting. In-depth interviews value participants’ lived experiences and are frequently used in phenomenology studies (as described in Chapter 6) .
When to use the different types of interview s
The type of interview a researcher uses should be determined by the study design, the research aims and objectives, and participant demographics. For example, if conducting a descriptive study, semi-structured interviews may be the best method of data collection. As explained in Chapter 5 , descriptive studies seek to describe phenomena, rather than to explain or interpret the data. A semi-structured interview, which seeks to expand upon some level of existing knowledge, will likely best facilitate this.
Similarly, if conducting a phenomenological study, in-depth interviews may be the best method of data collection. As described in Chapter 6 , the key concept of phenomenology is the individual. The emphasis is on the lived experience of that individual and the person’s sense-making of those experiences. Therefore, an in-depth interview is likely best placed to elicit that rich data.
While some interview types are better suited to certain study designs, there are no restrictions on the type of interview that may be used. For example, semi-structured interviews provide an excellent accompaniment to trial participation (see Chapter 11 about mixed methods), and key stakeholder interviews, as part of an action research study, can be used to define priorities, barriers and enablers to implementation.
How do I write my interview questions?
An interview aims to explore the experiences, understandings, opinions and motivations of research participants. The general rule is that the interviewee should speak for 80 per cent of the interview, and the interviewer should only be asking questions and clarifying responses, for about 20 per cent of the interview. This percentage may differ depending on the interview type; for example, a semi-structured interview involves the researcher asking more questions than in an in-depth interview. Still, to facilitate free-flowing responses, it is important to use open-ended language to encourage participants to be expansive in their responses. Examples of open-ended terms include questions that start with ‘who’, ‘how’ and ‘where’.
The researcher should avoid closed-ended questions that can be answered with yes or no, and limit conversation. For example, asking a participant ‘Did you have this experience?’ can elicit a simple ‘yes’, whereas asking them to ‘Describe your experience’, will likely encourage a narrative response. Table 13.1 provides examples of terminology to include and avoid in developing interview questions.
Table 13.1. Interview question formats to use and avoid
| Use | Avoid |
|---|---|
| Tell me about… | Do you think that… |
| What happened when… | Will you do this… |
| Why is this important? | Did you believe that… |
| How did you feel when…How do you… | Were there issues from your perspective… |
| What are the…What does... |
How long should my interview be?
There is no rule about how long an interview should take. Different types of interviews will likely run for different periods of time, but this also depends on the research question/s and the type of participant. For example, given that a semi-structured interview is seeking to expand on some previous knowledge, the interview may need no longer than 30 minutes, or up to one hour. An in-depth interview seeks to explore a topic in a greater level of detail and therefore, at a minimum, would be expected to last an hour. A dyad interview may be as short as 15 minutes (e.g. if the dyad is a person with dementia and a family member or caregiver) or longer, depending on the pairing.
Designing your interview guide
To figure out what questions to ask in an interview guide, the researcher may consult the literature, speak to experts (including people with lived experience) about the research and draw on their current knowledge. The topics and questions should be mapped to the research question/s, and the interview guide should be developed well in advance of commencing data collection. This enables time and opportunity to pilot-test the interview guide. The pilot interview provides an opportunity to explore the language and clarity of questions, the order and flow of the guide and to determine whether the instructions are clear to participants both before and after the interview. It can be beneficial to pilot-test the interview guide with someone who is not familiar with the research topic, to make sure that the language used is easily understood (and will be by participants, too). The study design should be used to determine the number of questions asked and the duration of the interview should guide the extent of the interview guide. The participant type may also determine the extent of the interview guide; for example, clinicians tend to be time-poor and therefore shorter, focused interviews are optimal. An interview guide is also likely to be shorter for a descriptive study than a phenomenological or ethnographic study, given the level of detail required. Chapter 5 outlined a descriptive study in which participants who had undergone percutaneous coronary intervention were interviewed. The interview guide consisted of four main questions and subsequent probing questions, linked to the research questions (see Table 13.2). 17
Table 13.2. Interview guide for a descriptive study
| Research question | Open questions | Probing questions and topics |
|---|---|---|
| How does the patient feel, physically and psychologically, after their procedure? | From your perspective, what would be considered a successful outcome of the procedure? | Did the procedure meet your expectations? How do you define whether the procedure was successful? |
| How did you feel after the procedure?
| How did you feel one week after the procedure and how does that compare with how you feel now? | |
| How does the patient function after their procedure? | After your procedure, tell me about your ability to do your daily activities? | Prompt for activities including gardening, housework, personal care, work-related and family-related tasks.Did you attend cardiac rehabilitation? Can you tell us about your experience of cardiac rehabilitation? What effect has medication had on your recovery?
|
| What are the long-term effects of the procedure? | What, if any, lifestyle changes have you made since your procedure? |
Table 13.3 is an example of a larger and more detailed interview guide, designed for the qualitative component of a mixed-methods study aiming to examine the work and financial effects of living with arthritis as a younger person. The questions are mapped to the World Health Organization’s International Classification of Functioning, Disability, and Health, which measures health and disability at individual and population levels. 18
Table 13.3. Detailed interview guide
| Research questions | Open questions | Probing questions |
|---|---|---|
| How do young people experience their arthritis diagnosis? | Tell me about your experience of being diagnosed with arthritis.How did being diagnosed with arthritis make you feel?Tell me about your experience of arthritis flare ups what do they feel like?What impacts arthritis flare ups or feeling like your arthritis is worse?What circumstances lead to these feelings?Based on your experience, what do you think causes symptoms of arthritis to become worse? | When were you diagnosed with arthritis?What type of arthritis were you diagnosed with?Does anyone else in your family have arthritis? What relation are they to you? |
| What are the work impacts of arthritis on younger people? | What is your field of work, and how long have you been in this role?How frequently do you work (full-time/part-time/casual)? | How has arthritis affected your work-related demands or career? How so?Has arthritis led you to reconsider your career? How so?Has arthritis affected your usual working hours each week? How so?How have changes to work or career because of your arthritis impacted other areas of life, i.e. mental health or family role? |
| What are the financial impacts of living with arthritis as a younger person? | Has your arthritis led to any financial concerns? | Financial concerns pertaining to:• Direct costs: rheumatologist, prescribed and non-prescribed medications (as well as supplements), allied health costs (rheumatology, physiotherapy, chiropractic, osteopathy, myotherapy), Pilates, and gym/personal trainer fees, complementary therapies.• Indirect costs: workplace absenteeism, productivity, loss of wages, informal care, cost of different types of insurance: health insurance (joint replacements) |
It is important to create an interview guide, for the following reasons:
- The researcher should be familiar with their research questions.
- Using an interview guide will enable the incorporation of feedback from the piloting process.
- It is difficult to predict how participants will respond to interview questions. They may answer in a way that is anticipated or they may provide unanticipated insights that warrant follow-up. An interview guide (a physical or digital copy) enables the researcher to note these answers and follow-up with appropriate inquiry.
- Participants will likely have provided heterogeneous answers to certain questions. The interview guide enables the researcher to note similarities and differences across various interviews, which may be important in data analysis.
- Even experienced qualitative researchers get nervous before an interview! The interview guide provides a safety net if the researcher forgets their questions or needs to anticipate the next question.
Setting up the interview
In the past, most interviews were conducted in person or by telephone. Emerging technologies promote easier access to research participation (e.g. by people living in rural or remote communities, or for people with mobility limitations). Even in metropolitan settings, many interviews are now conducted electronically (e.g. using videoconferencing platforms). Regardless of your interview setting, it is essential that the interview environment is comfortable for the participant. This process can begin as soon as potential participants express interest in your research. Following are some tips from the literature and our own experiences of leading interviews:
- Answer questions and set clear expectations . Participating in research is not an everyday task. People do not necessarily know what to expect during a research interview, and this can be daunting. Give people as much information as possible, answer their questions about the research and set clear expectations about what the interview will entail and how long it is expected to last. Let them know that the interview will be recorded for transcription and analysis purposes. Consider sending the interview questions a few days before the interview. This gives people time and space to reflect on their experiences, consider their responses to questions and to provide informed consent for their participation.
- Consider your setting . If conducting the interview in person, consider the location and room in which the interview will be held. For example, if in a participant’s home, be mindful of their private space. Ask if you should remove your shoes before entering their home. If they offer refreshments (which in our experience many participants do), accept it with gratitude if possible. These considerations apply beyond the participant’s home; if using a room in an office setting, consider privacy and confidentiality, accessibility and potential for disruption. Consider the temperature as well as the furniture in the room, who may be able to overhear conversations and who may walk past. Similarly, if interviewing by phone or online, take time to assess the space, and if in a house or office that is not quiet or private, use headphones as needed.
- Build rapport. The research topic may be important to participants from a professional perspective, or they may have deep emotional connections to the topic of interest. Regardless of the nature of the interview, it is important to remember that participants are being asked to open up to an interviewer who is likely to be a stranger. Spend some time with participants before the interview, to make sure that they are comfortable. Engage in some general conversation, and ask if they have any questions before you start. Remember that it is not a normal part of someone’s day to participate in research. Make it an enjoyable and/or meaningful experience for them, and it will enhance the data that you collect.
- Let participants guide you. Oftentimes, the ways in which researchers and participants describe the same phenomena are different. In the interview, reflect the participant’s language. Make sure they feel heard and that they are willing and comfortable to speak openly about their experiences. For example, our research involves talking to older adults about their experience of falls. We noticed early in this research that participants did not use the word ‘fall’ but would rather use terms such as ‘trip’, ‘went over’ and ‘stumbled’. As interviewers we adopted the participant’s language into our questions.
- Listen consistently and express interest. An interview is more complex than a simple question-and-answer format. The best interview data comes from participants feeling comfortable and confident to share their stories. By the time you are completing the 20th interview, it can be difficult to maintain the same level of concentration as with the first interview. Try to stay engaged: nod along with your participants, maintain eye contact, murmur in agreement and sympathise where warranted.
- The interviewer is both the data collector and the data collection instrument. The data received is only as good as the questions asked. In qualitative research, the researcher influences how participants answer questions. It is important to remain reflexive and aware of how your language, body language and attitude might influence the interview. Being rested and prepared will enhance the quality of the questions asked and hence the data collected.
- Avoid excessive use of ‘why’. It can be challenging for participants to recall why they felt a certain way or acted in a particular manner. Try to avoid asking ‘why’ questions too often, and instead adopt some of the open language described earlier in the chapter.
After your interview
When you have completed your interview, thank the participant and let them know they can contact you if they have any questions or follow-up information they would like to provide. If the interview has covered sensitive topics or the participant has become distressed throughout the interview, make sure that appropriate referrals and follow-up are provided (see section 6).
Download the recording from your device and make sure it is saved in a secure location that can only be accessed by people on the approved research team (see Chapters 35 and 36).
It is important to know what to do immediately after each interview is completed. Interviews should be transcribed – that is, reproduced verbatim for data analysis. Transcribing data is an important step in the process of analysis, but it is very time-consuming; transcribing a 60-minute interview can take up to 8 hours. Data analysis is discussed in Section 4.
Table 13.4. Examples of the four types of interviews
| Title | ||||
|---|---|---|---|---|
| CC Licence | ||||
| First author and year | Cuthbertson, 2019 | Bannon, 2021 | McGranahan, 2020 | Gutierrez-Garcia, 2021 |
| Interview type | Key stakeholder | Dyad | Narrative | Life history |
| Interview guide | Appendix A | eAppendix Supplement | Not provided, but the text states that ‘qualitative semi-structured narrative interviews’ were conducted.’ [methods] | Not provided, but the text states that ‘an open and semi-structured question guide was designed for use.' [methods] |
| Study design | Convergent mixed-methods study | Qualitative dyadic study | Narrative interview study | Life history and lifeline techniques |
| Number of participants | 30Key stakeholders were emergency management or disaster healthcare practitioners, academics specialising in disaster management in the Oceania region, and policy managers. | 23 dyads | 28 | 7 |
| Aim | ‘To investigate threats to the health and well-being of societies associated with disaster impact in Oceania.’ [abstract] | ‘To explore the lived experiences of couples managing young-onset dementia using an integrated dyadic coping model.’[abstract] | ‘To explore the experiences and views of people with psychotic experiences who have not received any treatment or other support from mental health services for the past 5 years.’ [abstract] | ‘To analyse the use of life histories and lifelines in the study of female genital mutilation in the context of cross-cultural research in participants with different languages.’ [abstract] |
| Country | Australia, Fiji, Indonesia, Aotearoa New Zealand, Timor Leste and Tonga | United States | England | Spain |
| Length of interview | 45–60 minutes | 60 minutes | 40-120 minutes | 3 sessionsSession 1: life history interviewSession 2: Lifeline activity where participants used drawings to complement or enhance their interviewSession 3: The researchers and participants worked together to finalise the lifeline. The life history interviews ran for 40 – 60 minutes. The timing for sessions 2 and 3 is not provided. |
| Sample of interview questions from interview guide | 1. What do you believe are the top five disaster risks or threats in the Oceania region today?2. What disaster risks do you believe are emerging in the Oceania region over the next decade?3. Why do you think these are risks?4. What are the drivers of these risks?5. Do you have any suggestions on how we can improve disaster risk assessment?6. Are the current disaster risk plans and practices suited to the future disaster risks? If not, why? If not, what do you think needs to be done to improve them?7. What are the key areas of disaster practice that can enhance future community resilience to disaster risk?8. What are the barriers or inhibitors to facilitating this practice?9. What are the solutions or facilitators to enhancing community resilience?[Appendix A]
| 1. We like to start by learning more about what you each first noticed that prompted the evaluations you went through to get to the diagnosis.• Can you each tell me about the earliest symptoms you noticed?2. What are the most noticeable or troubling symptoms that you have experienced since the time of diagnosis?• How have your changes in functioning impacted you?• Emotionally, how do you feel about your symptoms and the changes in functioning you are experiencing?3. Are you open with your friends and family about the diagnosis?• Have you experienced any stigma related to your diagnosis?4. What is your understanding of the diagnosis?• What is your understanding about the how this condition will affect you both in the future? How are you getting information about this diagnosis?[eAppendix Supplement]
| Not provided. | Not provided. |
| Analysis | Thematic analysis guided by The Hazard and Peril Glossary for describing and categorising disasters applied by the Centre for Research on the Epidemiology of Disasters Emergency Events Database | Thematic analysis guided by the Dyadic Coping Theoretical Framework | Inductive thematic analysis outlined by Braun and Clarke. | Phenomenological method proposed by Giorgi (sense of the whole):1. Reading the entire description to obtain a general sense of the discourse2. The researcher goes back to the beginning and reads the text again, with the aim of distinguishing the meaning units by separating the perspective of the phenomenon of interest3. The researcher expresses the contents of the units of meaning more clearly by creating categories4. The researcher synthesises the units and categories of meaning into a consistent statement that takes into account the participant’s experience and language. |
| Main themes | 1. Climate change is observed as a contemporary and emerging disaster risk2. Risk is contextual to the different countries, communities and individuals in Oceania.3. Human development trajectories and their impact, along with perceptions of a changing world, are viewed as drivers of current and emerging risks.4. Current disaster risk plans and practices are not suited to future disaster risks.5. Increased education and education of risk and risk assessment at a local level to empower community risk ownership.[Results, Box 1] | 1. Stress communication2. Positive individual dyadic coping3. Positive conjoint dyadic coping4. Negative individual dyadic coping5. Negative conjoint dyadic coping[Abstract] | 1. Perceiving psychosis as positive2. Making sense of psychotic experiences3. Finding sources of strength4. Negative past experiences of mental health services5. Positive past experiences with individual clinicians[Abstract] | 1. Important moments and their relationship with female genital mutilation2. The ritual knife: how sharp or blunt it is at different stages, where and how women are subsequently held as a result3. Changing relationships with family: how being subject to female genital mutilation changed relationships with mothers4. Female genital mutilation increases the risk of future childbirth complications which change relationships with family and healthcare systems5. Managing experiences with early exposure to physical and sexual violence across the lifespan. |
Interviews are the most common data collection technique in qualitative research. There are four main types of interviews; the one you choose will depend on your research question, aims and objectives. It is important to formulate open-ended interview questions that are understandable and easy for participants to answer. Key considerations in setting up the interview will enhance the quality of the data obtained and the experience of the interview for the participant and the researcher.
- Gill P, Stewart K, Treasure E, Chadwick B. Methods of data collection in qualitative research: interviews and focus groups. Br Dent J . 2008;204(6):291-295. doi:10.1038/bdj.2008.192
- DeJonckheere M, Vaughn LM. Semistructured interviewing in primary care research: a balance of relationship and rigour. Fam Med Community Health . 2019;7(2):e000057. doi:10.1136/fmch-2018-000057
- Nyanchoka L, Tudur-Smith C, Porcher R, Hren D. Key stakeholders’ perspectives and experiences with defining, identifying and displaying gaps in health research: a qualitative study. BMJ Open . 2020;10(11):e039932. doi:10.1136/bmjopen-2020-039932
- Morgan DL, Ataie J, Carder P, Hoffman K. Introducing dyadic interviews as a method for collecting qualitative data. Qual Health Res . 2013;23(9):1276-84. doi:10.1177/1049732313501889
- Picchi S, Bonapitacola C, Borghi E, et al. The narrative interview in therapeutic education. The diabetic patients’ point of view. Acta Biomed . Jul 18 2018;89(6-S):43-50. doi:10.23750/abm.v89i6-S.7488
- Stuij M, Elling A, Abma T. Negotiating exercise as medicine: Narratives from people with type 2 diabetes. Health (London) . 2021;25(1):86-102. doi:10.1177/1363459319851545
- Buchmann M, Wermeling M, Lucius-Hoene G, Himmel W. Experiences of food abstinence in patients with type 2 diabetes: a qualitative study. BMJ Open . 2016;6(1):e008907. doi:10.1136/bmjopen-2015-008907
- Jessee E. The Life History Interview. Handbook of Research Methods in Health Social Sciences . 2018:1-17:Chapter 80-1.
- Sheftel A, Zembrzycki S. Only Human: A Reflection on the Ethical and Methodological Challenges of Working with “Difficult” Stories. The Oral History Review . 2019;37(2):191-214. doi:10.1093/ohr/ohq050
- Harnisch H, Montgomery E. “What kept me going”: A qualitative study of avoidant responses to war-related adversity and perpetration of violence by former forcibly recruited children and youth in the Acholi region of northern Uganda. Soc Sci Med . 2017;188:100-108. doi:10.1016/j.socscimed.2017.07.007
- Ruslin., Mashuri S, Rasak MSA, Alhabsyi M, Alhabsyi F, Syam H. Semi-structured Interview: A Methodological Reflection on the Development of a Qualitative Research Instrument in Educational Studies. IOSR-JRME . 2022;12(1):22-29. doi:10.9790/7388-1201052229
- Chang T, Llanes M, Gold KJ, Fetters MD. Perspectives about and approaches to weight gain in pregnancy: a qualitative study of physicians and nurse midwives. BMC Pregnancy & Childbirth . 2013;13(47)doi:10.1186/1471-2393-13-47
- DeJonckheere M, Robinson CH, Evans L, et al. Designing for Clinical Change: Creating an Intervention to Implement New Statin Guidelines in a Primary Care Clinic. JMIR Hum Factors . 2018;5(2):e19. doi:10.2196/humanfactors.9030
- Knott E, Rao AH, Summers K, Teeger C. Interviews in the social sciences. Nature Reviews Methods Primers . 2022;2(1)doi:10.1038/s43586-022-00150-6
- Bergenholtz H, Missel M, Timm H. Talking about death and dying in a hospital setting – a qualitative study of the wishes for end-of-life conversations from the perspective of patients and spouses. BMC Palliat Care . 2020;19(1):168. doi:10.1186/s12904-020-00675-1
- Olorunsaiye CZ, Degge HM, Ubanyi TO, Achema TA, Yaya S. “It’s like being involved in a car crash”: teen pregnancy narratives of adolescents and young adults in Jos, Nigeria. Int Health . 2022;14(6):562-571. doi:10.1093/inthealth/ihab069
- Ayton DR, Barker AL, Peeters G, et al. Exploring patient-reported outcomes following percutaneous coronary intervention: A qualitative study. Health Expect . 2018;21(2):457-465. doi:10.1111/hex.12636
- World Health Organization. International Classification of Functioning, Disability and Health (ICF). WHO. https://www.who.int/standards/classifications/international-classification-of-functioning-disability-and-health#:~:text=ICF%20is%20the%20WHO%20framework,and%20measure%20health%20and%20disability.
- Cuthbertson J, Rodriguez-Llanes JM, Robertson A, Archer F. Current and Emerging Disaster Risks Perceptions in Oceania: Key Stakeholders Recommendations for Disaster Management and Resilience Building. Int J Environ Res Public Health . 2019;16(3)doi:10.3390/ijerph16030460
- Bannon SM, Grunberg VA, Reichman M, et al. Thematic Analysis of Dyadic Coping in Couples With Young-Onset Dementia. JAMA Netw Open . 2021;4(4):e216111. doi:10.1001/jamanetworkopen.2021.6111
- McGranahan R, Jakaite Z, Edwards A, Rennick-Egglestone S, Slade M, Priebe S. Living with Psychosis without Mental Health Services: A Narrative Interview Study. BMJ Open . 2021;11(7):e045661. doi:10.1136/bmjopen-2020-045661
- Gutiérrez-García AI, Solano-Ruíz C, Siles-González J, Perpiñá-Galvañ J. Life Histories and Lifelines: A Methodological Symbiosis for the Study of Female Genital Mutilation. Int J Qual Methods . 2021;20doi:10.1177/16094069211040969
Qualitative Research – a practical guide for health and social care researchers and practitioners Copyright © 2023 by Danielle Berkovic is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License , except where otherwise noted.
Share This Book
- Harvard Library
- Research Guides
- Faculty of Arts & Sciences Libraries
Library Support for Qualitative Research
- Interview Research
General Handbooks and Overviews
Qualitative research communities.
- Types of Interviews
- Recruiting & Engaging Participants
- Interview Questions
- Conducting Interviews
- Recording & Transcription
- Data Analysis
- Managing Interview Data
- Finding Extant Interviews
- Past Workshops on Interview Research
- Methodological Resources
- Remote & Virtual Fieldwork
- Data Management & Repositories
- Campus Access
- Interviews as a Method for Qualitative Research (video) This short video summarizes why interviews can serve as useful data in qualitative research.
- InterViews by Steinar Kvale Interviewing is an essential tool in qualitative research and this introduction to interviewing outlines both the theoretical underpinnings and the practical aspects of the process. After examining the role of the interview in the research process, Steinar Kvale considers some of the key philosophical issues relating to interviewing: the interview as conversation, hermeneutics, phenomenology, concerns about ethics as well as validity, and postmodernism. Having established this framework, the author then analyzes the seven stages of the interview process - from designing a study to writing it up.
- Practical Evaluation by Michael Quinn Patton Surveys different interviewing strategies, from, a) informal/conversational, to b) interview guide approach, to c) standardized and open-ended, to d) closed/quantitative. Also discusses strategies for wording questions that are open-ended, clear, sensitive, and neutral, while supporting the speaker. Provides suggestions for probing and maintaining control of the interview process, as well as suggestions for recording and transcription.
- The SAGE Handbook of Interview Research by Amir B. Marvasti (Editor); James A. Holstein (Editor); Jaber F. Gubrium (Editor); Karyn D. McKinney (Editor) The new edition of this landmark volume emphasizes the dynamic, interactional, and reflexive dimensions of the research interview. Contributors highlight the myriad dimensions of complexity that are emerging as researchers increasingly frame the interview as a communicative opportunity as much as a data-gathering format. The book begins with the history and conceptual transformations of the interview, which is followed by chapters that discuss the main components of interview practice. Taken together, the contributions to The SAGE Handbook of Interview Research: The Complexity of the Craft encourage readers simultaneously to learn the frameworks and technologies of interviewing and to reflect on the epistemological foundations of the interview craft.
- International Congress of Qualitative Inquiry They host an annual confrerence at the University of Illinois at Urbana-Champaign, which aims to facilitate the development of qualitative research methods across a wide variety of academic disciplines, among other initiatives.
- METHODSPACE An online home of the research methods community, where practicing researchers share how to make research easier.
- Social Research Association, UK The SRA is the membership organisation for social researchers in the UK and beyond. It supports researchers via training, guidance, publications, research ethics, events, branches, and careers.
- Social Science Research Council The SSRC administers fellowships and research grants that support the innovation and evaluation of new policy solutions. They convene researchers and stakeholders to share evidence-based policy solutions and incubate new research agendas, produce online knowledge platforms and technical reports that catalog research-based policy solutions, and support mentoring programs that broaden problem-solving research opportunities.
- << Previous: Taguette
- Next: Types of Interviews >>
Except where otherwise noted, this work is subject to a Creative Commons Attribution 4.0 International License , which allows anyone to share and adapt our material as long as proper attribution is given. For details and exceptions, see the Harvard Library Copyright Policy ©2021 Presidents and Fellows of Harvard College.
Qualitative study design: Interviews
- Qualitative study design
- Phenomenology
- Grounded theory
- Ethnography
- Narrative inquiry
- Action research
- Case Studies
- Field research
- Focus groups
- Observation
- Surveys & questionnaires
- Study Designs Home
Interviews are intended to find out the experiences, understandings, opinions, or motivations of participants. The relationship between the interviewer and interviewee is crucial to the success of the research interview; the interviewer builds an environment of trust with the interviewee/s, guiding the interviewee/s through a set of topics or questions to be discussed in depth.
Interviews are the most commonly used qualitative data gathering technique and are used with grounded theory, focus groups, and case studies.
- Interviews are purposive conversations between the researcher and the interviewee, either alone or as part of a group
- Interviews can be face to face, via telecommunications (Skype, Facetime, or phone), or via email (internet or email interview)
- The length of an interview varies. They may be anywhere from thirty minutes to several hours in length, depending on your research approach
- Structured interviews use a set list of questions which need to be asked in order, increasing the reliability and credibility of the data but decreasing responsiveness to interviewee/s. Structured interviews are like a verbal survey
- Unstructured interviews are where the interviewer has a set list of topics to address but no predetermined questions. This increases the flexibility of the interview but decreases the reliability of the data. Unstructured interviews may be used in long-term field observation research
- Semi-structured interviews are the middle ground. Semi-structured interviews require the interviewer to have a list of questions and topics pre-prepared, which can be asked in different ways with different interviewee/s. Semi-structured interviews increase the flexibility and the responsiveness of the interview while keeping the interview on track, increasing the reliability and credibility of the data. Semi-structured interviews are one of the most common interview techniques.
- Flexible – probing questions can be asked, and the order of questions changed, depending on the participant and how structured or unstructured the interview is
- Quick way to collect data
- Familiarity – most interviewees are familiar with the concept of an interview and are comfortable with this research approach
Limitations
- Not all participants are equally articulate or perceptive
- Questions must be worded carefully to reduce response bias
- Transcription of interviews can be time and labour intensive
Example questions
- What are the experiences of midwives in providing care to high-risk mothers, where there is a history of drug or alcohol use?
Example studies
Sandelin, A., Kalman, S., Gustafsson, B. (2019). Prerequisites for safe intraoperative nursing care and teamwork – operating theatre nurses’ perspectives: a qualitative interview study, Journal of Clinical Nursing, 28, 2635-2643. Doi: 10.1111/jocn.14850
Babbie, E. (2008). The basics of social research (4th ed). Belmont: Thomson Wadsworth
Creswell, J.W. & Creswell, J.D. (2018). Research design: Qualitative, quantitative and mixed methods approaches (5th ed). Thousand Oaks: SAGE
Jamshed, S. (2014). Qualitative research method-interviewing and observation. Journal of basic and clinical pharmacy, 5(4), 87-88. doi:10.4103/0976-0105.141942
Lindlof, T. & Taylor, B. (2002). Qualitative communication research methods (2nd ed). Thousand Oaks: SAGE .
- << Previous: Surveys & questionnaires
- Next: Sampling >>
- Last Updated: Jul 3, 2024 11:46 AM
- URL: https://deakin.libguides.com/qualitative-study-designs
Root out friction in every digital experience, super-charge conversion rates, and optimise digital self-service
Uncover insights from any interaction, deliver AI-powered agent coaching, and reduce cost to serve
Increase revenue and loyalty with real-time insights and recommendations delivered straight to teams on the ground
Know how your people feel and empower managers to improve employee engagement, productivity, and retention
Take action in the moments that matter most along the employee journey and drive bottom line growth
Whatever they’re are saying, wherever they’re saying it, know exactly what’s going on with your people
Get faster, richer insights with qual and quant tools that make powerful market research available to everyone
Run concept tests, pricing studies, prototyping + more with fast, powerful studies designed by UX research experts
Track your brand performance 24/7 and act quickly to respond to opportunities and challenges in your market
Meet the operating system for experience management
- Free Account
- Product Demos
- For Digital
- For Customer Care
- For Human Resources
- For Researchers
- Financial Services
- All Industries
Popular Use Cases
- Customer Experience
- Employee Experience
- Employee Exit Interviews
- Net Promoter Score
- Voice of Customer
- Customer Success Hub
- Product Documentation
- Training & Certification
- XM Institute
- Popular Resources
- Customer Stories
- Artificial Intelligence
Market Research
- Partnerships
- Marketplace
The annual gathering of the experience leaders at the world’s iconic brands building breakthrough business results.
- English/AU & NZ
- Español/Europa
- Español/América Latina
- Português Brasileiro
- REQUEST DEMO
- Experience Management
- Ultimate Guide to Market Research
- Qualitative Research Interviews
Try Qualtrics for free
How to carry out great interviews in qualitative research.
11 min read An interview is one of the most versatile methods used in qualitative research. Here’s what you need to know about conducting great qualitative interviews.
What is a qualitative research interview?
Qualitative research interviews are a mainstay among q ualitative research techniques, and have been in use for decades either as a primary data collection method or as an adjunct to a wider research process. A qualitative research interview is a one-to-one data collection session between a researcher and a participant. Interviews may be carried out face-to-face, over the phone or via video call using a service like Skype or Zoom.
There are three main types of qualitative research interview – structured, unstructured or semi-structured.
- Structured interviews Structured interviews are based around a schedule of predetermined questions and talking points that the researcher has developed. At their most rigid, structured interviews may have a precise wording and question order, meaning that they can be replicated across many different interviewers and participants with relatively consistent results.
- Unstructured interviews Unstructured interviews have no predetermined format, although that doesn’t mean they’re ad hoc or unplanned. An unstructured interview may outwardly resemble a normal conversation, but the interviewer will in fact be working carefully to make sure the right topics are addressed during the interaction while putting the participant at ease with a natural manner.
- Semi-structured interviews Semi-structured interviews are the most common type of qualitative research interview, combining the informality and rapport of an unstructured interview with the consistency and replicability of a structured interview. The researcher will come prepared with questions and topics, but will not need to stick to precise wording. This blended approach can work well for in-depth interviews.
Free eBook: The qualitative research design handbook
What are the pros and cons of interviews in qualitative research?
As a qualitative research method interviewing is hard to beat, with applications in social research, market research, and even basic and clinical pharmacy. But like any aspect of the research process, it’s not without its limitations. Before choosing qualitative interviewing as your research method, it’s worth weighing up the pros and cons.
Pros of qualitative interviews:
- provide in-depth information and context
- can be used effectively when their are low numbers of participants
- provide an opportunity to discuss and explain questions
- useful for complex topics
- rich in data – in the case of in-person or video interviews , the researcher can observe body language and facial expression as well as the answers to questions
Cons of qualitative interviews:
- can be time-consuming to carry out
- costly when compared to some other research methods
- because of time and cost constraints, they often limit you to a small number of participants
- difficult to standardise your data across different researchers and participants unless the interviews are very tightly structured
- As the Open University of Hong Kong notes, qualitative interviews may take an emotional toll on interviewers
Qualitative interview guides
Semi-structured interviews are based on a qualitative interview guide, which acts as a road map for the researcher. While conducting interviews, the researcher can use the interview guide to help them stay focused on their research questions and make sure they cover all the topics they intend to.
An interview guide may include a list of questions written out in full, or it may be a set of bullet points grouped around particular topics. It can prompt the interviewer to dig deeper and ask probing questions during the interview if appropriate.
Consider writing out the project’s research question at the top of your interview guide, ahead of the interview questions. This may help you steer the interview in the right direction if it threatens to head off on a tangent.
Avoid bias in qualitative research interviews
According to Duke University , bias can create significant problems in your qualitative interview.
- Acquiescence bias is common to many qualitative methods, including focus groups. It occurs when the participant feels obliged to say what they think the researcher wants to hear. This can be especially problematic when there is a perceived power imbalance between participant and interviewer. To counteract this, Duke University’s experts recommend emphasising the participant’s expertise in the subject being discussed, and the value of their contributions.
- Interviewer bias is when the interviewer’s own feelings about the topic come to light through hand gestures, facial expressions or turns of phrase. Duke’s recommendation is to stick to scripted phrases where this is an issue, and to make sure researchers become very familiar with the interview guide or script before conducting interviews, so that they can hone their delivery.
What kinds of questions should you ask in a qualitative interview?
The interview questions you ask need to be carefully considered both before and during the data collection process. As well as considering the topics you’ll cover, you will need to think carefully about the way you ask questions.
Open-ended interview questions – which cannot be answered with a ‘yes’ ‘no’ or ‘maybe’ – are recommended by many researchers as a way to pursue in depth information.
An example of an open-ended question is “What made you want to move to the East Coast?” This will prompt the participant to consider different factors and select at least one. Having thought about it carefully, they may give you more detailed information about their reasoning.
A closed-ended question , such as “Would you recommend your neighbourhood to a friend?” can be answered without too much deliberation, and without giving much information about personal thoughts, opinions and feelings.
Follow-up questions can be used to delve deeper into the research topic and to get more detail from open-ended questions. Examples of follow-up questions include:
- What makes you say that?
- What do you mean by that?
- Can you tell me more about X?
- What did/does that mean to you?
As well as avoiding closed-ended questions, be wary of leading questions. As with other qualitative research techniques such as surveys or focus groups, these can introduce bias in your data. Leading questions presume a certain point of view shared by the interviewer and participant, and may even suggest a foregone conclusion.
An example of a leading question might be: “You moved to New York in 1990, didn’t you?” In answering the question, the participant is much more likely to agree than disagree. This may be down to acquiescence bias or a belief that the interviewer has checked the information and already knows the correct answer.
Other leading questions involve adjectival phrases or other wording that introduces negative or positive connotations about a particular topic. An example of this kind of leading question is: “Many employees dislike wearing masks to work. How do you feel about this?” It presumes a positive opinion and the participant may be swayed by it, or not want to contradict the interviewer.
Harvard University’s guidelines for qualitative interview research add that you shouldn’t be afraid to ask embarrassing questions – “if you don’t ask, they won’t tell.” Bear in mind though that too much probing around sensitive topics may cause the interview participant to withdraw. The Harvard guidelines recommend leaving sensitive questions til the later stages of the interview when a rapport has been established.
More tips for conducting qualitative interviews
Observing a participant’s body language can give you important data about their thoughts and feelings. It can also help you decide when to broach a topic, and whether to use a follow-up question or return to the subject later in the interview.
Be conscious that the participant may regard you as the expert, not themselves. In order to make sure they express their opinions openly, use active listening skills like verbal encouragement and paraphrasing and clarifying their meaning to show how much you value what they are saying.
Remember that part of the goal is to leave the interview participant feeling good about volunteering their time and their thought process to your research. Aim to make them feel empowered , respected and heard.
Unstructured interviews can demand a lot of a researcher, both cognitively and emotionally. Be sure to leave time in between in-depth interviews when scheduling your data collection to make sure you maintain the quality of your data, as well as your own well-being .
Recording and transcribing interviews
Historically, recording qualitative research interviews and then transcribing the conversation manually would have represented a significant part of the cost and time involved in research projects that collect qualitative data.
Fortunately, researchers now have access to digital recording tools, and even speech-to-text technology that can automatically transcribe interview data using AI and machine learning. This type of tool can also be used to capture qualitative data from qualitative research (focus groups,ect.) making this kind of social research or market research much less time consuming.
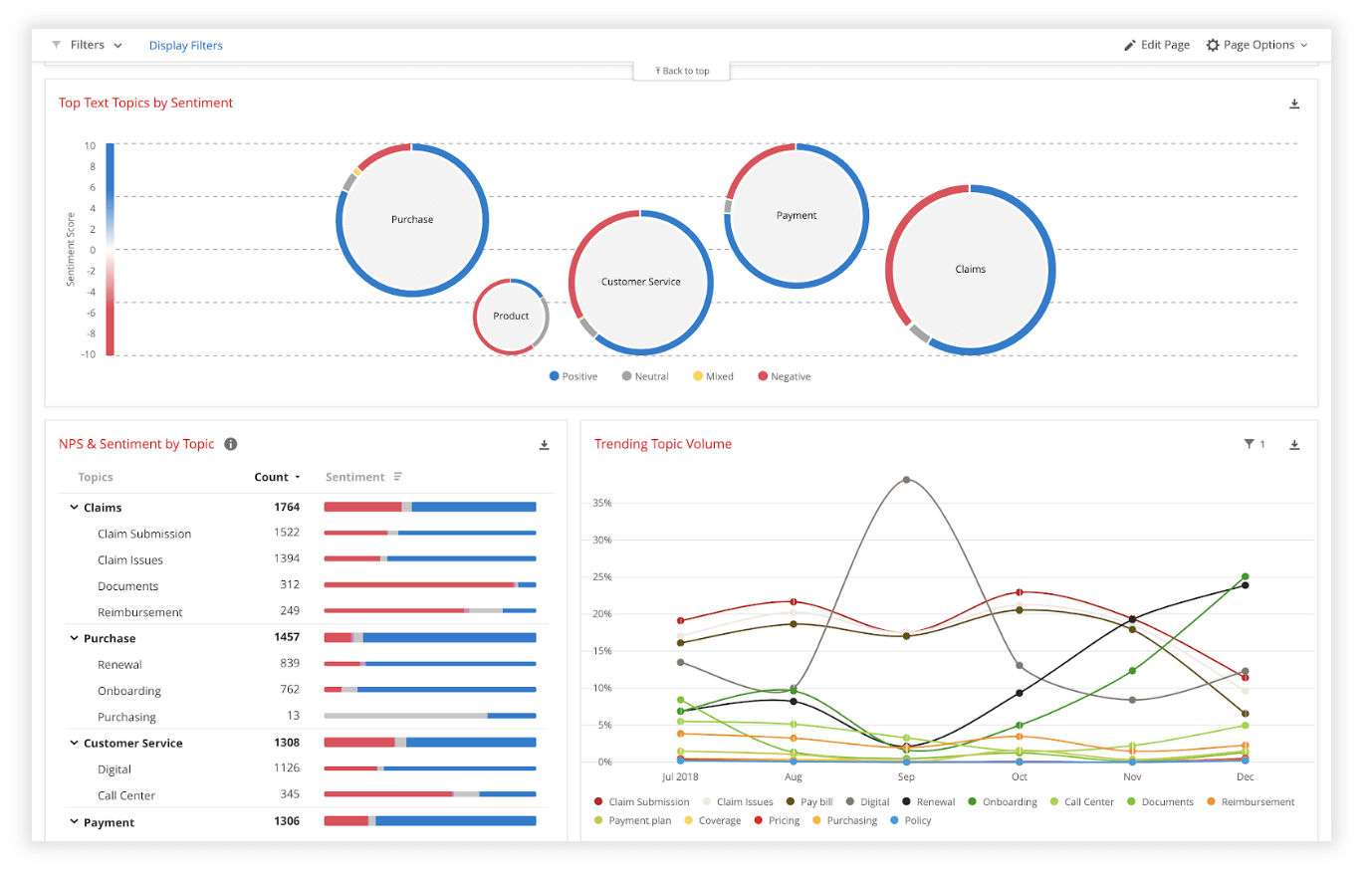
Data analysis
Qualitative interview data is unstructured, rich in content and difficult to analyse without the appropriate tools. Fortunately, machine learning and AI can once again make things faster and easier when you use qualitative methods like the research interview.
Text analysis tools and natural language processing software can ‘read’ your transcripts and voice data and identify patterns and trends across large volumes of text or speech. They can also perform khttps://www.qualtrics.com/experience-management/research/sentiment-analysis/
which assesses overall trends in opinion and provides an unbiased overall summary of how participants are feeling.
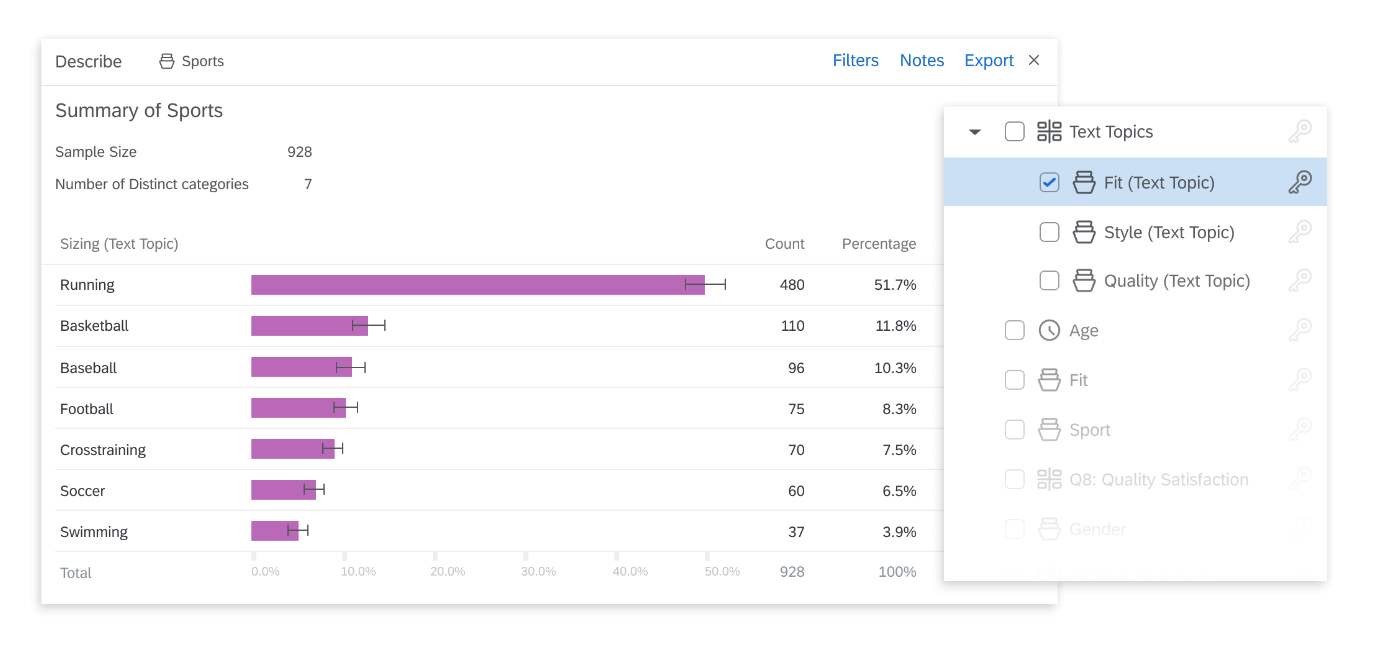
Another feature of text analysis tools is their ability to categorise information by topic, sorting it into groupings that help you organise your data according to the topic discussed.
All in all, interviews are a valuable technique for qualitative research in business, yielding rich and detailed unstructured data. Historically, they have only been limited by the human capacity to interpret and communicate results and conclusions, which demands considerable time and skill.
When you combine this data with AI tools that can interpret it quickly and automatically, it becomes easy to analyse and structure, dovetailing perfectly with your other business data. An additional benefit of natural language analysis tools is that they are free of subjective biases, and can replicate the same approach across as much data as you choose. By combining human research skills with machine analysis, qualitative research methods such as interviews are more valuable than ever to your business.
Related resources
Video in qualitative research 10 min read, descriptive research 8 min read, market intelligence 9 min read, qualitative research questions 11 min read, ethnographic research 11 min read, business research methods 12 min read, qualitative research design 12 min read, request demo.
Ready to learn more about Qualtrics?

The Ultimate Guide to Qualitative Research - Part 1: The Basics

- Introduction and overview
- What is qualitative research?
- What is qualitative data?
- Examples of qualitative data
- Qualitative vs. quantitative research
- Mixed methods
- Qualitative research preparation
- Theoretical perspective
- Theoretical framework
- Literature reviews
- Research question
- Conceptual framework
- Conceptual vs. theoretical framework
- Data collection
- Qualitative research methods
- Introduction
What is an interview and its purpose in qualitative research?
What are some examples of interviews in research, how to carry out great interviews in qualitative research, fundamental types of interviews, process of conducting an interview.
- Focus groups
- Observational research
- Case studies
- Ethnographical research
Ethical considerations
- Confidentiality and privacy
- Power dynamics
- Reflexivity
Interviews: Research methods and approaches
As a qualitative research method, interviewing is widely used to gather in-depth information from participants about their experiences, opinions, and perspectives on a specific topic. There are various qualitative research techniques for interviews available to researchers to achieve the greatest potential in data collection .

This section will provide an overview of the importance of interviews, the different types of interviews, tools for conducting interviews, analysis of interview data , and ethical considerations in this research method. Note that the focus group interview is a related concept but will be discussed in greater detail in the next section of this guide, as focus groups have slightly different dynamics to consider.
Interviews, as a qualitative research method , play a pivotal role in uncovering complexities in human behavior and decision-making. Researchers can observe behavior, on the one hand, or they can investigate the perspectives and values informing that behavior by interviewing research participants.
Purpose and importance
Interviews allow researchers to delve into the subjective experiences of individuals, providing insights that may not be accessible through other research methods. They illuminate people's perceptions, thoughts, feelings, and understandings about a particular phenomenon. Data representing these views can form the foundation for identifying recurring themes regarding that phenomenon.
Unlike quantitative methods, which typically collect numerical data that can be statistically analyzed, interviews capture rich, detailed data in the form of words, ideas, and themes. They allow researchers to collect data on people's experiences in a manner that is sensitive to the context and the individual's perspective. Through interviews, researchers can explore the meanings people attribute to their experiences and gain a deeper understanding of the phenomena being studied.
Interviews also empower participants by giving them a voice. The interviewee has the opportunity to express their views, feelings, and experiences in their own words. This participatory aspect of interviews underscores the respect for individual experiences and perspectives, which is a central tenet of qualitative research.
Comparing interviews with other methods
While interviews share many similarities with other qualitative methods, they also have unique features that set them apart. Unlike interviews, methods like observations are more passive and rely more on the researcher's interpretation of events.
On the other hand, interviews actively involve participants in the data generation process. Compared to surveys , which may limit responses to predetermined choices or word limits, interviews allow for open-ended responses and the flexibility to explore topics in depth.
However, it's worth noting that interviews do not have to be a stand-alone method. They are often used with other methods, such as observation or document analysis , in a multi-method or mixed-methods research design . This combination of methods can enhance the richness and credibility of the data collected, providing a more holistic understanding of the research problem.
The qualitative research interview can be conducted in various formats, each with its own strengths and limitations. Choosing the appropriate type of interview to use largely depends on the research question, the nature of the topic, the characteristics of the participants, and the resources available to the researcher.
Face-to-face interviews
In-person interviews are often considered the traditional form of interviewing. They involve a direct conversation between the interviewer and the interviewee. This form allows for comprehensive communication as it includes verbal and non-verbal cues such as body language, facial expressions, and tone of voice.

This type of interview allows for immediate clarification of responses and can help foster rapport between the interviewer and interviewee, which may lead to richer, more nuanced data. However, these kinds of interviews can be time-consuming, expensive, and limited by geographic location.
Telephone interviews
Telephone interviews can be a practical alternative when face-to-face interviews are not feasible due to distance, time, or budget constraints. Phone interviews allow researchers to reach participants who may be geographically dispersed and offer a level of anonymity that may encourage candid responses, particularly on sensitive topics.
However, they might lack non-verbal cues that can provide additional context to a participant's responses. A phone interview may differ from a conversation in person in that you can't see someone's face, gestures, or other body language, which might be useful for contextualizing detailed information.
Online/internet-based interviews
Online or internet-based interviews conducted through platforms such as Zoom, Skype, or email have become increasingly popular in recent years. They can be synchronous (occurring in real-time, like video calls) or asynchronous (participants respond in their own time, such as email interviews).

These interviews can reach participants globally, are often cost-effective, and can be more convenient for both the researcher and the participant. However, they rely on technology and internet access, which may not be available to all potential participants.

Effective interview research with ATLAS.ti
Get key insights from insightful analysis with ATLAS.ti. Try a free trial today.
Qualitative interviews are more than just casual conversations. Some qualitative research interviews may not follow a strict structure and allow the researcher to explore any topics in the moment. In contrast, other interviews may be highly structured and aim to collect the same kind of information across participants. As a matter of empirical research, research interviews require careful planning, execution, and reflection to ensure they yield valuable and trustworthy data. Here are some key components to consider:
Developing appropriate interview questions
The foundation of any successful interview lies in its questions. Good interview questions are open-ended, clear, and directly related to the research objectives. They should allow participants to share their experiences, opinions, and feelings without leading them toward certain answers. In qualitative research, it's often useful to have a mix of more and less structured questions, allowing for both depth and breadth in responses.
Building rapport with participants
Establishing rapport with interviewees is crucial to encourage open and honest responses. In-depth interviews can be challenging if the interviewer doesn't know the interviewee in detail or hasn't established the necessary trust.

Researchers establish rapport with interviewees by displaying empathy, active listening, and respect. Clarifying the purpose of the interview, ensuring confidentiality, and asking for consent before beginning can also help in building trust.
Note-taking and recording
Accurate and comprehensive documentation of interview data is critical. While audio or video recording is highly recommended for completeness and accuracy, it's also beneficial to take notes during or immediately after the interview. These notes can capture non-verbal cues, the interviewer's impressions, and any issues or incidents that occur during the interview.
Ethical considerations are paramount in any research involving human participants. Researchers must obtain informed consent , respect participants' privacy and confidentiality , and ensure participants understand their right to withdraw from the study at any time without any negative consequences. It's also important to be aware of power dynamics and strive for a respectful and equitable researcher-participant relationship.
The effectiveness of a qualitative interview largely depends on the thoughtfulness and rigor with which these components are addressed. Interviews are not just a data collection tool; they are a way of acknowledging and respecting participants' lived experiences and perspectives. Therefore, each component should be handled with utmost care and consideration.
Organize your data all in one place.
Text files, PDFs, videos, and pictures. ATLAS.ti helps you analyze them all. See how with a free trial.
The structure of an interview can greatly influence the data collected. The level of structure varies along a continuum, with structured and unstructured interviews occupying opposite ends of that spectrum.
Unstructured interviews
Unstructured interviews are characterized by their flexibility. The researcher usually only has a list of topics or themes to be covered, known as an interview guide, but the conversation does not follow a predetermined set of questions. Instead, the interviewer allows the conversation to flow naturally, following leads provided by the interviewee. An unstructured interview is particularly useful when the researcher is exploring a new area of study and aims to gather as much information as possible without preconceived notions.
Semi-structured interviews
Semi-structured interviews strike a balance between flexibility and structure. The researcher has a list of predetermined questions to conduct interviews but is free to ask additional open-ended questions or to deviate from the list based on the interviewee's responses. The semi-structured interview is the most common form of interview in qualitative research, as it provides deep, rich data while still ensuring that all necessary topics are covered.

Structured interviews
Structured interviews , sometimes called standardized interviews, are the most rigid form of interview. The researcher asks the same set of predetermined questions in the same order to all participants, with little to no deviation.
While a structured interview may limit the depth of data collected, it allows for greater consistency across interviews. This can be helpful for keeping responses confined to the research topic and comparing responses between participants.
In determining the level of structure for an interview, researchers should consider their research objectives, the nature of the topic, and the characteristics of the participants. Different structures lend themselves to different research goals, and the most effective interviewers are those who can adapt their approach based on the needs of their study.
Conducting an interview in qualitative research involves a series of well-planned steps before, during, and after the interview. These steps ensure that the process is systematic, ethical, and capable of yielding high-quality data.
Pre-interview preparation and research
Before conducting the interview, the researcher needs to thoroughly understand the research topic, define the purpose of the interview, and identify potential interviewees. Preparing an interview guide with key themes or questions is essential, though the level of detail will depend on the interview structure. Logistics, such as scheduling the interview at a convenient time and place for the participant and ensuring necessary equipment is available and working, also need to be addressed.
Conducting the interview
The interview begins with an introduction in which the interviewer explains the purpose of the interview, assures confidentiality, and obtains consent from the participant. Throughout the interview, the researcher should aim to build rapport, listen attentively, and adapt their questioning based on the interviewee's responses. Non-verbal cues should also be observed and noted, as they can provide additional insights.
Post-interview activities
After the interview, it is important to thank the participant for their time and contribution. Researchers should then promptly transcribe the interview while the details are still fresh. Reflections and observations about the interview should also be noted, including the context, the behavior of the participant, and any unexpected occurrences. These notes can provide valuable context during data analysis.
Executing each of these stages effectively requires not only good planning and organization but also interpersonal skills, flexibility, and respect for the participant. The quality of the data collected during an interview is largely dependent on how well the interview process is managed.
Transcribing interviews
The transcription of interview data is a critical step in the qualitative research process. This involves converting the recorded audio or video interviews into written text, providing a detailed account of the dialogues that took place during the interviews.

Transcriptions allow for more detailed examination, analysis, and reporting of the data. However, making transcriptions can be arduous and time-consuming. Here are some key considerations in the transcription process:
Types of transcription
There are two main types of transcription: verbatim and clean. Verbatim transcription involves writing down every single word, pause, and utterance made during the interview. This is a very detailed and time-consuming process, but it can be useful when the researcher needs to analyze not just the content of the interview but also the way it was expressed. On the other hand, clean transcription omits irrelevant elements like stutters, repetitions, and filler words, focusing instead on the core content of the conversation.
Manual vs. automated transcription
Researchers may choose to transcribe interviews manually or use transcription software. Manual transcription, while time-consuming, allows researchers to become intimately familiar with the data and can be more accurate, especially for complex or nuanced dialogues.
Automated transcription software, however, can save time and effort, particularly for large volumes of data, although it may require manual checking and correction for errors. Some researchers choose a hybrid approach, using software for the initial transcription and then manually checking and correcting the output.
Formatting and anonymizing transcripts
To facilitate analysis, transcripts should be formatted consistently, with clear identifiers for different speakers and timestamps for reference. If there are multiple interviewers or participants, each individual's speech should be clearly marked. Additionally, to ensure confidentiality, any personally identifiable information should be removed or anonymized in the transcript. This is especially important to consider in qualitative data, because participants may talk about aspects of their lives through which they could be identified, for instance if they mention specific names, their neighborhood, or place of work.
Quality checks
Finally, it's important to check the quality of the transcript. This could involve a second person checking the transcription against the audio or the researcher re-listening to portions of the recording to confirm accuracy. Any unclear or inaudible sections should be marked in the transcript.

Get the most out of interviews with ATLAS.ti
Collect, transcribe, and analyze interviews with our intuitive interface. Try it out with a free trial.

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- J Basic Clin Pharm
- v.5(4); September 2014-November 2014
Qualitative research method-interviewing and observation
Shazia jamshed.
Department of Pharmacy Practice, Kulliyyah of Pharmacy, International Islamic University Malaysia, Kuantan Campus, Pahang, Malaysia
Buckley and Chiang define research methodology as “a strategy or architectural design by which the researcher maps out an approach to problem-finding or problem-solving.”[ 1 ] According to Crotty, research methodology is a comprehensive strategy ‘that silhouettes our choice and use of specific methods relating them to the anticipated outcomes,[ 2 ] but the choice of research methodology is based upon the type and features of the research problem.[ 3 ] According to Johnson et al . mixed method research is “a class of research where the researcher mixes or combines quantitative and qualitative research techniques, methods, approaches, theories and or language into a single study.[ 4 ] In order to have diverse opinions and views, qualitative findings need to be supplemented with quantitative results.[ 5 ] Therefore, these research methodologies are considered to be complementary to each other rather than incompatible to each other.[ 6 ]
Qualitative research methodology is considered to be suitable when the researcher or the investigator either investigates new field of study or intends to ascertain and theorize prominent issues.[ 6 , 7 ] There are many qualitative methods which are developed to have an in depth and extensive understanding of the issues by means of their textual interpretation and the most common types are interviewing and observation.[ 7 ]
Interviewing
This is the most common format of data collection in qualitative research. According to Oakley, qualitative interview is a type of framework in which the practices and standards be not only recorded, but also achieved, challenged and as well as reinforced.[ 8 ] As no research interview lacks structure[ 9 ] most of the qualitative research interviews are either semi-structured, lightly structured or in-depth.[ 9 ] Unstructured interviews are generally suggested in conducting long-term field work and allow respondents to let them express in their own ways and pace, with minimal hold on respondents’ responses.[ 10 ]
Pioneers of ethnography developed the use of unstructured interviews with local key informants that is., by collecting the data through observation and record field notes as well as to involve themselves with study participants. To be precise, unstructured interview resembles a conversation more than an interview and is always thought to be a “controlled conversation,” which is skewed towards the interests of the interviewer.[ 11 ] Non-directive interviews, form of unstructured interviews are aimed to gather in-depth information and usually do not have pre-planned set of questions.[ 11 ] Another type of the unstructured interview is the focused interview in which the interviewer is well aware of the respondent and in times of deviating away from the main issue the interviewer generally refocuses the respondent towards key subject.[ 11 ] Another type of the unstructured interview is an informal, conversational interview, based on unplanned set of questions that are generated instantaneously during the interview.[ 11 ]
In contrast, semi-structured interviews are those in-depth interviews where the respondents have to answer preset open-ended questions and thus are widely employed by different healthcare professionals in their research. Semi-structured, in-depth interviews are utilized extensively as interviewing format possibly with an individual or sometimes even with a group.[ 6 ] These types of interviews are conducted once only, with an individual or with a group and generally cover the duration of 30 min to more than an hour.[ 12 ] Semi-structured interviews are based on semi-structured interview guide, which is a schematic presentation of questions or topics and need to be explored by the interviewer.[ 12 ] To achieve optimum use of interview time, interview guides serve the useful purpose of exploring many respondents more systematically and comprehensively as well as to keep the interview focused on the desired line of action.[ 12 ] The questions in the interview guide comprise of the core question and many associated questions related to the central question, which in turn, improve further through pilot testing of the interview guide.[ 7 ] In order to have the interview data captured more effectively, recording of the interviews is considered an appropriate choice but sometimes a matter of controversy among the researcher and the respondent. Hand written notes during the interview are relatively unreliable, and the researcher might miss some key points. The recording of the interview makes it easier for the researcher to focus on the interview content and the verbal prompts and thus enables the transcriptionist to generate “verbatim transcript” of the interview.
Similarly, in focus groups, invited groups of people are interviewed in a discussion setting in the presence of the session moderator and generally these discussions last for 90 min.[ 7 ] Like every research technique having its own merits and demerits, group discussions have some intrinsic worth of expressing the opinions openly by the participants. On the contrary in these types of discussion settings, limited issues can be focused, and this may lead to the generation of fewer initiatives and suggestions about research topic.
Observation
Observation is a type of qualitative research method which not only included participant's observation, but also covered ethnography and research work in the field. In the observational research design, multiple study sites are involved. Observational data can be integrated as auxiliary or confirmatory research.[ 11 ]
Research can be visualized and perceived as painstaking methodical efforts to examine, investigate as well as restructure the realities, theories and applications. Research methods reflect the approach to tackling the research problem. Depending upon the need, research method could be either an amalgam of both qualitative and quantitative or qualitative or quantitative independently. By adopting qualitative methodology, a prospective researcher is going to fine-tune the pre-conceived notions as well as extrapolate the thought process, analyzing and estimating the issues from an in-depth perspective. This could be carried out by one-to-one interviews or as issue-directed discussions. Observational methods are, sometimes, supplemental means for corroborating research findings.
Thank you for visiting nature.com. You are using a browser version with limited support for CSS. To obtain the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in Internet Explorer). In the meantime, to ensure continued support, we are displaying the site without styles and JavaScript.
- View all journals
- Explore content
- About the journal
- Publish with us
- Sign up for alerts
- Published: 05 October 2018
Interviews and focus groups in qualitative research: an update for the digital age
- P. Gill 1 &
- J. Baillie 2
British Dental Journal volume 225 , pages 668–672 ( 2018 ) Cite this article
32k Accesses
63 Citations
20 Altmetric
Metrics details
Highlights that qualitative research is used increasingly in dentistry. Interviews and focus groups remain the most common qualitative methods of data collection.
Suggests the advent of digital technologies has transformed how qualitative research can now be undertaken.
Suggests interviews and focus groups can offer significant, meaningful insight into participants' experiences, beliefs and perspectives, which can help to inform developments in dental practice.
Qualitative research is used increasingly in dentistry, due to its potential to provide meaningful, in-depth insights into participants' experiences, perspectives, beliefs and behaviours. These insights can subsequently help to inform developments in dental practice and further related research. The most common methods of data collection used in qualitative research are interviews and focus groups. While these are primarily conducted face-to-face, the ongoing evolution of digital technologies, such as video chat and online forums, has further transformed these methods of data collection. This paper therefore discusses interviews and focus groups in detail, outlines how they can be used in practice, how digital technologies can further inform the data collection process, and what these methods can offer dentistry.
You have full access to this article via your institution.
Similar content being viewed by others

Interviews in the social sciences

Professionalism in dentistry: deconstructing common terminology
A review of technical and quality assessment considerations of audio-visual and web-conferencing focus groups in qualitative health research, introduction.
Traditionally, research in dentistry has primarily been quantitative in nature. 1 However, in recent years, there has been a growing interest in qualitative research within the profession, due to its potential to further inform developments in practice, policy, education and training. Consequently, in 2008, the British Dental Journal (BDJ) published a four paper qualitative research series, 2 , 3 , 4 , 5 to help increase awareness and understanding of this particular methodological approach.
Since the papers were originally published, two scoping reviews have demonstrated the ongoing proliferation in the use of qualitative research within the field of oral healthcare. 1 , 6 To date, the original four paper series continue to be well cited and two of the main papers remain widely accessed among the BDJ readership. 2 , 3 The potential value of well-conducted qualitative research to evidence-based practice is now also widely recognised by service providers, policy makers, funding bodies and those who commission, support and use healthcare research.
Besides increasing standalone use, qualitative methods are now also routinely incorporated into larger mixed method study designs, such as clinical trials, as they can offer additional, meaningful insights into complex problems that simply could not be provided by quantitative methods alone. Qualitative methods can also be used to further facilitate in-depth understanding of important aspects of clinical trial processes, such as recruitment. For example, Ellis et al . investigated why edentulous older patients, dissatisfied with conventional dentures, decline implant treatment, despite its established efficacy, and frequently refuse to participate in related randomised clinical trials, even when financial constraints are removed. 7 Through the use of focus groups in Canada and the UK, the authors found that fears of pain and potential complications, along with perceived embarrassment, exacerbated by age, are common reasons why older patients typically refuse dental implants. 7
The last decade has also seen further developments in qualitative research, due to the ongoing evolution of digital technologies. These developments have transformed how researchers can access and share information, communicate and collaborate, recruit and engage participants, collect and analyse data and disseminate and translate research findings. 8 Where appropriate, such technologies are therefore capable of extending and enhancing how qualitative research is undertaken. 9 For example, it is now possible to collect qualitative data via instant messaging, email or online/video chat, using appropriate online platforms.
These innovative approaches to research are therefore cost-effective, convenient, reduce geographical constraints and are often useful for accessing 'hard to reach' participants (for example, those who are immobile or socially isolated). 8 , 9 However, digital technologies are still relatively new and constantly evolving and therefore present a variety of pragmatic and methodological challenges. Furthermore, given their very nature, their use in many qualitative studies and/or with certain participant groups may be inappropriate and should therefore always be carefully considered. While it is beyond the scope of this paper to provide a detailed explication regarding the use of digital technologies in qualitative research, insight is provided into how such technologies can be used to facilitate the data collection process in interviews and focus groups.
In light of such developments, it is perhaps therefore timely to update the main paper 3 of the original BDJ series. As with the previous publications, this paper has been purposely written in an accessible style, to enhance readability, particularly for those who are new to qualitative research. While the focus remains on the most common qualitative methods of data collection – interviews and focus groups – appropriate revisions have been made to provide a novel perspective, and should therefore be helpful to those who would like to know more about qualitative research. This paper specifically focuses on undertaking qualitative research with adult participants only.
Overview of qualitative research
Qualitative research is an approach that focuses on people and their experiences, behaviours and opinions. 10 , 11 The qualitative researcher seeks to answer questions of 'how' and 'why', providing detailed insight and understanding, 11 which quantitative methods cannot reach. 12 Within qualitative research, there are distinct methodologies influencing how the researcher approaches the research question, data collection and data analysis. 13 For example, phenomenological studies focus on the lived experience of individuals, explored through their description of the phenomenon. Ethnographic studies explore the culture of a group and typically involve the use of multiple methods to uncover the issues. 14
While methodology is the 'thinking tool', the methods are the 'doing tools'; 13 the ways in which data are collected and analysed. There are multiple qualitative data collection methods, including interviews, focus groups, observations, documentary analysis, participant diaries, photography and videography. Two of the most commonly used qualitative methods are interviews and focus groups, which are explored in this article. The data generated through these methods can be analysed in one of many ways, according to the methodological approach chosen. A common approach is thematic data analysis, involving the identification of themes and subthemes across the data set. Further information on approaches to qualitative data analysis has been discussed elsewhere. 1
Qualitative research is an evolving and adaptable approach, used by different disciplines for different purposes. Traditionally, qualitative data, specifically interviews, focus groups and observations, have been collected face-to-face with participants. In more recent years, digital technologies have contributed to the ongoing evolution of qualitative research. Digital technologies offer researchers different ways of recruiting participants and collecting data, and offer participants opportunities to be involved in research that is not necessarily face-to-face.
Research interviews are a fundamental qualitative research method 15 and are utilised across methodological approaches. Interviews enable the researcher to learn in depth about the perspectives, experiences, beliefs and motivations of the participant. 3 , 16 Examples include, exploring patients' perspectives of fear/anxiety triggers in dental treatment, 17 patients' experiences of oral health and diabetes, 18 and dental students' motivations for their choice of career. 19
Interviews may be structured, semi-structured or unstructured, 3 according to the purpose of the study, with less structured interviews facilitating a more in depth and flexible interviewing approach. 20 Structured interviews are similar to verbal questionnaires and are used if the researcher requires clarification on a topic; however they produce less in-depth data about a participant's experience. 3 Unstructured interviews may be used when little is known about a topic and involves the researcher asking an opening question; 3 the participant then leads the discussion. 20 Semi-structured interviews are commonly used in healthcare research, enabling the researcher to ask predetermined questions, 20 while ensuring the participant discusses issues they feel are important.
Interviews can be undertaken face-to-face or using digital methods when the researcher and participant are in different locations. Audio-recording the interview, with the consent of the participant, is essential for all interviews regardless of the medium as it enables accurate transcription; the process of turning the audio file into a word-for-word transcript. This transcript is the data, which the researcher then analyses according to the chosen approach.
Types of interview
Qualitative studies often utilise one-to-one, face-to-face interviews with research participants. This involves arranging a mutually convenient time and place to meet the participant, signing a consent form and audio-recording the interview. However, digital technologies have expanded the potential for interviews in research, enabling individuals to participate in qualitative research regardless of location.
Telephone interviews can be a useful alternative to face-to-face interviews and are commonly used in qualitative research. They enable participants from different geographical areas to participate and may be less onerous for participants than meeting a researcher in person. 15 A qualitative study explored patients' perspectives of dental implants and utilised telephone interviews due to the quality of the data that could be yielded. 21 The researcher needs to consider how they will audio record the interview, which can be facilitated by purchasing a recorder that connects directly to the telephone. One potential disadvantage of telephone interviews is the inability of the interviewer and researcher to see each other. This is resolved using software for audio and video calls online – such as Skype – to conduct interviews with participants in qualitative studies. Advantages of this approach include being able to see the participant if video calls are used, enabling observation of non-verbal communication, and the software can be free to use. However, participants are required to have a device and internet connection, as well as being computer literate, potentially limiting who can participate in the study. One qualitative study explored the role of dental hygienists in reducing oral health disparities in Canada. 22 The researcher conducted interviews using Skype, which enabled dental hygienists from across Canada to be interviewed within the research budget, accommodating the participants' schedules. 22
A less commonly used approach to qualitative interviews is the use of social virtual worlds. A qualitative study accessed a social virtual world – Second Life – to explore the health literacy skills of individuals who use social virtual worlds to access health information. 23 The researcher created an avatar and interview room, and undertook interviews with participants using voice and text methods. 23 This approach to recruitment and data collection enables individuals from diverse geographical locations to participate, while remaining anonymous if they wish. Furthermore, for interviews conducted using text methods, transcription of the interview is not required as the researcher can save the written conversation with the participant, with the participant's consent. However, the researcher and participant need to be familiar with how the social virtual world works to engage in an interview this way.
Conducting an interview
Ensuring informed consent before any interview is a fundamental aspect of the research process. Participants in research must be afforded autonomy and respect; consent should be informed and voluntary. 24 Individuals should have the opportunity to read an information sheet about the study, ask questions, understand how their data will be stored and used, and know that they are free to withdraw at any point without reprisal. The qualitative researcher should take written consent before undertaking the interview. In a face-to-face interview, this is straightforward: the researcher and participant both sign copies of the consent form, keeping one each. However, this approach is less straightforward when the researcher and participant do not meet in person. A recent protocol paper outlined an approach for taking consent for telephone interviews, which involved: audio recording the participant agreeing to each point on the consent form; the researcher signing the consent form and keeping a copy; and posting a copy to the participant. 25 This process could be replicated in other interview studies using digital methods.
There are advantages and disadvantages of using face-to-face and digital methods for research interviews. Ultimately, for both approaches, the quality of the interview is determined by the researcher. 16 Appropriate training and preparation are thus required. Healthcare professionals can use their interpersonal communication skills when undertaking a research interview, particularly questioning, listening and conversing. 3 However, the purpose of an interview is to gain information about the study topic, 26 rather than offering help and advice. 3 The researcher therefore needs to listen attentively to participants, enabling them to describe their experience without interruption. 3 The use of active listening skills also help to facilitate the interview. 14 Spradley outlined elements and strategies for research interviews, 27 which are a useful guide for qualitative researchers:
Greeting and explaining the project/interview
Asking descriptive (broad), structural (explore response to descriptive) and contrast (difference between) questions
Asymmetry between the researcher and participant talking
Expressing interest and cultural ignorance
Repeating, restating and incorporating the participant's words when asking questions
Creating hypothetical situations
Asking friendly questions
Knowing when to leave.
For semi-structured interviews, a topic guide (also called an interview schedule) is used to guide the content of the interview – an example of a topic guide is outlined in Box 1 . The topic guide, usually based on the research questions, existing literature and, for healthcare professionals, their clinical experience, is developed by the research team. The topic guide should include open ended questions that elicit in-depth information, and offer participants the opportunity to talk about issues important to them. This is vital in qualitative research where the researcher is interested in exploring the experiences and perspectives of participants. It can be useful for qualitative researchers to pilot the topic guide with the first participants, 10 to ensure the questions are relevant and understandable, and amending the questions if required.
Regardless of the medium of interview, the researcher must consider the setting of the interview. For face-to-face interviews, this could be in the participant's home, in an office or another mutually convenient location. A quiet location is preferable to promote confidentiality, enable the researcher and participant to concentrate on the conversation, and to facilitate accurate audio-recording of the interview. For interviews using digital methods the same principles apply: a quiet, private space where the researcher and participant feel comfortable and confident to participate in an interview.
Box 1: Example of a topic guide
Study focus: Parents' experiences of brushing their child's (aged 0–5) teeth
1. Can you tell me about your experience of cleaning your child's teeth?
How old was your child when you started cleaning their teeth?
Why did you start cleaning their teeth at that point?
How often do you brush their teeth?
What do you use to brush their teeth and why?
2. Could you explain how you find cleaning your child's teeth?
Do you find anything difficult?
What makes cleaning their teeth easier for you?
3. How has your experience of cleaning your child's teeth changed over time?
Has it become easier or harder?
Have you changed how often and how you clean their teeth? If so, why?
4. Could you describe how your child finds having their teeth cleaned?
What do they enjoy about having their teeth cleaned?
Is there anything they find upsetting about having their teeth cleaned?
5. Where do you look for information/advice about cleaning your child's teeth?
What did your health visitor tell you about cleaning your child's teeth? (If anything)
What has the dentist told you about caring for your child's teeth? (If visited)
Have any family members given you advice about how to clean your child's teeth? If so, what did they tell you? Did you follow their advice?
6. Is there anything else you would like to discuss about this?
Focus groups
A focus group is a moderated group discussion on a pre-defined topic, for research purposes. 28 , 29 While not aligned to a particular qualitative methodology (for example, grounded theory or phenomenology) as such, focus groups are used increasingly in healthcare research, as they are useful for exploring collective perspectives, attitudes, behaviours and experiences. Consequently, they can yield rich, in-depth data and illuminate agreement and inconsistencies 28 within and, where appropriate, between groups. Examples include public perceptions of dental implants and subsequent impact on help-seeking and decision making, 30 and general dental practitioners' views on patient safety in dentistry. 31
Focus groups can be used alone or in conjunction with other methods, such as interviews or observations, and can therefore help to confirm, extend or enrich understanding and provide alternative insights. 28 The social interaction between participants often results in lively discussion and can therefore facilitate the collection of rich, meaningful data. However, they are complex to organise and manage, due to the number of participants, and may also be inappropriate for exploring particularly sensitive issues that many participants may feel uncomfortable about discussing in a group environment.
Focus groups are primarily undertaken face-to-face but can now also be undertaken online, using appropriate technologies such as email, bulletin boards, online research communities, chat rooms, discussion forums, social media and video conferencing. 32 Using such technologies, data collection can also be synchronous (for example, online discussions in 'real time') or, unlike traditional face-to-face focus groups, asynchronous (for example, online/email discussions in 'non-real time'). While many of the fundamental principles of focus group research are the same, regardless of how they are conducted, a number of subtle nuances are associated with the online medium. 32 Some of which are discussed further in the following sections.
Focus group considerations
Some key considerations associated with face-to-face focus groups are: how many participants are required; should participants within each group know each other (or not) and how many focus groups are needed within a single study? These issues are much debated and there is no definitive answer. However, the number of focus groups required will largely depend on the topic area, the depth and breadth of data needed, the desired level of participation required 29 and the necessity (or not) for data saturation.
The optimum group size is around six to eight participants (excluding researchers) but can work effectively with between three and 14 participants. 3 If the group is too small, it may limit discussion, but if it is too large, it may become disorganised and difficult to manage. It is, however, prudent to over-recruit for a focus group by approximately two to three participants, to allow for potential non-attenders. For many researchers, particularly novice researchers, group size may also be informed by pragmatic considerations, such as the type of study, resources available and moderator experience. 28 Similar size and mix considerations exist for online focus groups. Typically, synchronous online focus groups will have around three to eight participants but, as the discussion does not happen simultaneously, asynchronous groups may have as many as 10–30 participants. 33
The topic area and potential group interaction should guide group composition considerations. Pre-existing groups, where participants know each other (for example, work colleagues) may be easier to recruit, have shared experiences and may enjoy a familiarity, which facilitates discussion and/or the ability to challenge each other courteously. 3 However, if there is a potential power imbalance within the group or if existing group norms and hierarchies may adversely affect the ability of participants to speak freely, then 'stranger groups' (that is, where participants do not already know each other) may be more appropriate. 34 , 35
Focus group management
Face-to-face focus groups should normally be conducted by two researchers; a moderator and an observer. 28 The moderator facilitates group discussion, while the observer typically monitors group dynamics, behaviours, non-verbal cues, seating arrangements and speaking order, which is essential for transcription and analysis. The same principles of informed consent, as discussed in the interview section, also apply to focus groups, regardless of medium. However, the consent process for online discussions will probably be managed somewhat differently. For example, while an appropriate participant information leaflet (and consent form) would still be required, the process is likely to be managed electronically (for example, via email) and would need to specifically address issues relating to technology (for example, anonymity and use, storage and access to online data). 32
The venue in which a face to face focus group is conducted should be of a suitable size, private, quiet, free from distractions and in a collectively convenient location. It should also be conducted at a time appropriate for participants, 28 as this is likely to promote attendance. As with interviews, the same ethical considerations apply (as discussed earlier). However, online focus groups may present additional ethical challenges associated with issues such as informed consent, appropriate access and secure data storage. Further guidance can be found elsewhere. 8 , 32
Before the focus group commences, the researchers should establish rapport with participants, as this will help to put them at ease and result in a more meaningful discussion. Consequently, researchers should introduce themselves, provide further clarity about the study and how the process will work in practice and outline the 'ground rules'. Ground rules are designed to assist, not hinder, group discussion and typically include: 3 , 28 , 29
Discussions within the group are confidential to the group
Only one person can speak at a time
All participants should have sufficient opportunity to contribute
There should be no unnecessary interruptions while someone is speaking
Everyone can be expected to be listened to and their views respected
Challenging contrary opinions is appropriate, but ridiculing is not.
Moderating a focus group requires considered management and good interpersonal skills to help guide the discussion and, where appropriate, keep it sufficiently focused. Avoid, therefore, participating, leading, expressing personal opinions or correcting participants' knowledge 3 , 28 as this may bias the process. A relaxed, interested demeanour will also help participants to feel comfortable and promote candid discourse. Moderators should also prevent the discussion being dominated by any one person, ensure differences of opinions are discussed fairly and, if required, encourage reticent participants to contribute. 3 Asking open questions, reflecting on significant issues, inviting further debate, probing responses accordingly, and seeking further clarification, as and where appropriate, will help to obtain sufficient depth and insight into the topic area.
Moderating online focus groups requires comparable skills, particularly if the discussion is synchronous, as the discussion may be dominated by those who can type proficiently. 36 It is therefore important that sufficient time and respect is accorded to those who may not be able to type as quickly. Asynchronous discussions are usually less problematic in this respect, as interactions are less instant. However, moderating an asynchronous discussion presents additional challenges, particularly if participants are geographically dispersed, as they may be online at different times. Consequently, the moderator will not always be present and the discussion may therefore need to occur over several days, which can be difficult to manage and facilitate and invariably requires considerable flexibility. 32 It is also worth recognising that establishing rapport with participants via online medium is often more challenging than via face-to-face and may therefore require additional time, skills, effort and consideration.
As with research interviews, focus groups should be guided by an appropriate interview schedule, as discussed earlier in the paper. For example, the schedule will usually be informed by the review of the literature and study aims, and will merely provide a topic guide to help inform subsequent discussions. To provide a verbatim account of the discussion, focus groups must be recorded, using an audio-recorder with a good quality multi-directional microphone. While videotaping is possible, some participants may find it obtrusive, 3 which may adversely affect group dynamics. The use (or not) of a video recorder, should therefore be carefully considered.
At the end of the focus group, a few minutes should be spent rounding up and reflecting on the discussion. 28 Depending on the topic area, it is possible that some participants may have revealed deeply personal issues and may therefore require further help and support, such as a constructive debrief or possibly even referral on to a relevant third party. It is also possible that some participants may feel that the discussion did not adequately reflect their views and, consequently, may no longer wish to be associated with the study. 28 Such occurrences are likely to be uncommon, but should they arise, it is important to further discuss any concerns and, if appropriate, offer them the opportunity to withdraw (including any data relating to them) from the study. Immediately after the discussion, researchers should compile notes regarding thoughts and ideas about the focus group, which can assist with data analysis and, if appropriate, any further data collection.
Qualitative research is increasingly being utilised within dental research to explore the experiences, perspectives, motivations and beliefs of participants. The contributions of qualitative research to evidence-based practice are increasingly being recognised, both as standalone research and as part of larger mixed-method studies, including clinical trials. Interviews and focus groups remain commonly used data collection methods in qualitative research, and with the advent of digital technologies, their utilisation continues to evolve. However, digital methods of qualitative data collection present additional methodological, ethical and practical considerations, but also potentially offer considerable flexibility to participants and researchers. Consequently, regardless of format, qualitative methods have significant potential to inform important areas of dental practice, policy and further related research.
Gussy M, Dickson-Swift V, Adams J . A scoping review of qualitative research in peer-reviewed dental publications. Int J Dent Hygiene 2013; 11 : 174–179.
Article Google Scholar
Burnard P, Gill P, Stewart K, Treasure E, Chadwick B . Analysing and presenting qualitative data. Br Dent J 2008; 204 : 429–432.
Gill P, Stewart K, Treasure E, Chadwick B . Methods of data collection in qualitative research: interviews and focus groups. Br Dent J 2008; 204 : 291–295.
Gill P, Stewart K, Treasure E, Chadwick B . Conducting qualitative interviews with school children in dental research. Br Dent J 2008; 204 : 371–374.
Stewart K, Gill P, Chadwick B, Treasure E . Qualitative research in dentistry. Br Dent J 2008; 204 : 235–239.
Masood M, Thaliath E, Bower E, Newton J . An appraisal of the quality of published qualitative dental research. Community Dent Oral Epidemiol 2011; 39 : 193–203.
Ellis J, Levine A, Bedos C et al. Refusal of implant supported mandibular overdentures by elderly patients. Gerodontology 2011; 28 : 62–68.
Macfarlane S, Bucknall T . Digital Technologies in Research. In Gerrish K, Lathlean J (editors) The Research Process in Nursing . 7th edition. pp. 71–86. Oxford: Wiley Blackwell; 2015.
Google Scholar
Lee R, Fielding N, Blank G . Online Research Methods in the Social Sciences: An Editorial Introduction. In Fielding N, Lee R, Blank G (editors) The Sage Handbook of Online Research Methods . pp. 3–16. London: Sage Publications; 2016.
Creswell J . Qualitative inquiry and research design: Choosing among five designs . Thousand Oaks, CA: Sage, 1998.
Guest G, Namey E, Mitchell M . Qualitative research: Defining and designing In Guest G, Namey E, Mitchell M (editors) Collecting Qualitative Data: A Field Manual For Applied Research . pp. 1–40. London: Sage Publications, 2013.
Chapter Google Scholar
Pope C, Mays N . Qualitative research: Reaching the parts other methods cannot reach: an introduction to qualitative methods in health and health services research. BMJ 1995; 311 : 42–45.
Giddings L, Grant B . A Trojan Horse for positivism? A critique of mixed methods research. Adv Nurs Sci 2007; 30 : 52–60.
Hammersley M, Atkinson P . Ethnography: Principles in Practice . London: Routledge, 1995.
Oltmann S . Qualitative interviews: A methodological discussion of the interviewer and respondent contexts Forum Qualitative Sozialforschung/Forum: Qualitative Social Research. 2016; 17 : Art. 15.
Patton M . Qualitative Research and Evaluation Methods . Thousand Oaks, CA: Sage, 2002.
Wang M, Vinall-Collier K, Csikar J, Douglas G . A qualitative study of patients' views of techniques to reduce dental anxiety. J Dent 2017; 66 : 45–51.
Lindenmeyer A, Bowyer V, Roscoe J, Dale J, Sutcliffe P . Oral health awareness and care preferences in patients with diabetes: a qualitative study. Fam Pract 2013; 30 : 113–118.
Gallagher J, Clarke W, Wilson N . Understanding the motivation: a qualitative study of dental students' choice of professional career. Eur J Dent Educ 2008; 12 : 89–98.
Tod A . Interviewing. In Gerrish K, Lacey A (editors) The Research Process in Nursing . Oxford: Blackwell Publishing, 2006.
Grey E, Harcourt D, O'Sullivan D, Buchanan H, Kipatrick N . A qualitative study of patients' motivations and expectations for dental implants. Br Dent J 2013; 214 : 10.1038/sj.bdj.2012.1178.
Farmer J, Peressini S, Lawrence H . Exploring the role of the dental hygienist in reducing oral health disparities in Canada: A qualitative study. Int J Dent Hygiene 2017; 10.1111/idh.12276.
McElhinney E, Cheater F, Kidd L . Undertaking qualitative health research in social virtual worlds. J Adv Nurs 2013; 70 : 1267–1275.
Health Research Authority. UK Policy Framework for Health and Social Care Research. Available at https://www.hra.nhs.uk/planning-and-improving-research/policies-standards-legislation/uk-policy-framework-health-social-care-research/ (accessed September 2017).
Baillie J, Gill P, Courtenay P . Knowledge, understanding and experiences of peritonitis among patients, and their families, undertaking peritoneal dialysis: A mixed methods study protocol. J Adv Nurs 2017; 10.1111/jan.13400.
Kvale S . Interviews . Thousand Oaks (CA): Sage, 1996.
Spradley J . The Ethnographic Interview . New York: Holt, Rinehart and Winston, 1979.
Goodman C, Evans C . Focus Groups. In Gerrish K, Lathlean J (editors) The Research Process in Nursing . pp. 401–412. Oxford: Wiley Blackwell, 2015.
Shaha M, Wenzell J, Hill E . Planning and conducting focus group research with nurses. Nurse Res 2011; 18 : 77–87.
Wang G, Gao X, Edward C . Public perception of dental implants: a qualitative study. J Dent 2015; 43 : 798–805.
Bailey E . Contemporary views of dental practitioners' on patient safety. Br Dent J 2015; 219 : 535–540.
Abrams K, Gaiser T . Online Focus Groups. In Field N, Lee R, Blank G (editors) The Sage Handbook of Online Research Methods . pp. 435–450. London: Sage Publications, 2016.
Poynter R . The Handbook of Online and Social Media Research . West Sussex: John Wiley & Sons, 2010.
Kevern J, Webb C . Focus groups as a tool for critical social research in nurse education. Nurse Educ Today 2001; 21 : 323–333.
Kitzinger J, Barbour R . Introduction: The Challenge and Promise of Focus Groups. In Barbour R S K J (editor) Developing Focus Group Research . pp. 1–20. London: Sage Publications, 1999.
Krueger R, Casey M . Focus Groups: A Practical Guide for Applied Research. 4th ed. Thousand Oaks, California: SAGE; 2009.
Download references
Author information
Authors and affiliations.
Senior Lecturer (Adult Nursing), School of Healthcare Sciences, Cardiff University,
Lecturer (Adult Nursing) and RCBC Wales Postdoctoral Research Fellow, School of Healthcare Sciences, Cardiff University,
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to P. Gill .
Rights and permissions
Reprints and permissions
About this article
Cite this article.
Gill, P., Baillie, J. Interviews and focus groups in qualitative research: an update for the digital age. Br Dent J 225 , 668–672 (2018). https://doi.org/10.1038/sj.bdj.2018.815
Download citation
Accepted : 02 July 2018
Published : 05 October 2018
Issue Date : 12 October 2018
DOI : https://doi.org/10.1038/sj.bdj.2018.815
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
This article is cited by
Assessment of women’s needs and wishes regarding interprofessional guidance on oral health in pregnancy – a qualitative study.
- Merle Ebinghaus
- Caroline Johanna Agricola
- Birgit-Christiane Zyriax
BMC Pregnancy and Childbirth (2024)
Translating brand reputation into equity from the stakeholder’s theory: an approach to value creation based on consumer’s perception & interactions
- Olukorede Adewole
International Journal of Corporate Social Responsibility (2024)
Perceptions and beliefs of community gatekeepers about genomic risk information in African cleft research
- Abimbola M. Oladayo
- Oluwakemi Odukoya
- Azeez Butali
BMC Public Health (2024)
Assessment of women’s needs, wishes and preferences regarding interprofessional guidance on nutrition in pregnancy – a qualitative study
‘baby mamas’ in urban ghana: an exploratory qualitative study on the factors influencing serial fathering among men in accra, ghana.
- Rosemond Akpene Hiadzi
- Jemima Akweley Agyeman
- Godwin Banafo Akrong
Reproductive Health (2023)
Quick links
- Explore articles by subject
- Guide to authors
- Editorial policies

Choosing an Interview Type for Qualitative Research
If you are conducting a qualitative study, you may be wondering what is the best interview type for qualitative research? Well, the answer is that it depends on your research design and what you want to accomplish. Let us start with the different types of interviews. There are three types of interviews: unstructured, semistructured, and structured.
Unstructured Interviews
These are interviews that take place with few, if any, interview questions. They often progress in the manner a normal conversation would, however it concerns the research topic under review. It is a relatively formless interview style that researchers use to establish rapport and comfort with the participant, and is extremely helpful when researchers are discussing sensitive topics. The researcher is expected to probe participants in order to obtain the most rich and in-depth information possible. If you select this interview style, just keep in mind that you may have to conduct several rounds of interviews with your participants in order to gather all the information you need. Since you do not use a standard interview protocol, sometimes participant’s narratives maneuver the conversation away from other aspects of the research topic you want to explore; it is a part of the conversational style this interview method requires.
Semistructured Interviews
These are interviews that use an interview protocol to help guide the researcher through the interview process. While this can incorporate conversational aspects, it is mostly a guided conversation between the researcher and participant. It does maintain some structure (hence the name semistructured), but it also provides the researcher with the ability to probe the participant for additional details. If you decide to choose this interview method, understand that it offers a great deal of flexibility for you as a researcher. You do not have to worry about needing to conduct several rounds of interviews because your interview protocol will keep you focused on gathering all the information that you need to answer your research question. Even though that is the goal with an interview protocol, there may be a need for additional probing so that you can get more details about participants’ thoughts, feelings, and opinions.
Need help with your Qualitative Research?
Schedule a time to speak with an expert using the calendar below.
Structured Interviews
These are interviews that strictly adhere to the use of an interview protocol to guide the researcher. It is a more rigid interview style, in that only the questions on the interview protocol are asked. As a result, there are not a lot of opportunities to probe and further explore topics that participants bring up when answering the interview questions. This method can be advantageous when researchers have a comprehensive list of interview questions, since it helps target the specific phenomenon or experience that the researcher is investigating. It makes for expedient interviewing and will gather the correct information that you need, so there should not be much need for you to do follow-up interviews for missed or forgotten questions.
Each interview type has its advantages and its disadvantages, as briefly outlined above. Selecting one depends on your research design and what you want to get out of your interviews. If you take some time to review your research design, this will help you determine which interview type works best for your study.
Looking for an easy to use qualitative analysis tool? Check out Intellectus Qualitative , the ultimate platform designed to redefine your qualitative research experience. Whether you’re a novice student researcher, a faculty member, or an experienced researcher, you’ve discovered a tool that combines simplicity with the power of AI.
Have a language expert improve your writing
Run a free plagiarism check in 10 minutes, generate accurate citations for free.
- Knowledge Base
Methodology
- What Is Qualitative Research? | Methods & Examples
What Is Qualitative Research? | Methods & Examples
Published on June 19, 2020 by Pritha Bhandari . Revised on June 22, 2023.
Qualitative research involves collecting and analyzing non-numerical data (e.g., text, video, or audio) to understand concepts, opinions, or experiences. It can be used to gather in-depth insights into a problem or generate new ideas for research.
Qualitative research is the opposite of quantitative research , which involves collecting and analyzing numerical data for statistical analysis.
Qualitative research is commonly used in the humanities and social sciences, in subjects such as anthropology, sociology, education, health sciences, history, etc.
- How does social media shape body image in teenagers?
- How do children and adults interpret healthy eating in the UK?
- What factors influence employee retention in a large organization?
- How is anxiety experienced around the world?
- How can teachers integrate social issues into science curriculums?
Table of contents
Approaches to qualitative research, qualitative research methods, qualitative data analysis, advantages of qualitative research, disadvantages of qualitative research, other interesting articles, frequently asked questions about qualitative research.
Qualitative research is used to understand how people experience the world. While there are many approaches to qualitative research, they tend to be flexible and focus on retaining rich meaning when interpreting data.
Common approaches include grounded theory, ethnography , action research , phenomenological research, and narrative research. They share some similarities, but emphasize different aims and perspectives.
| Approach | What does it involve? |
|---|---|
| Grounded theory | Researchers collect rich data on a topic of interest and develop theories . |
| Researchers immerse themselves in groups or organizations to understand their cultures. | |
| Action research | Researchers and participants collaboratively link theory to practice to drive social change. |
| Phenomenological research | Researchers investigate a phenomenon or event by describing and interpreting participants’ lived experiences. |
| Narrative research | Researchers examine how stories are told to understand how participants perceive and make sense of their experiences. |
Note that qualitative research is at risk for certain research biases including the Hawthorne effect , observer bias , recall bias , and social desirability bias . While not always totally avoidable, awareness of potential biases as you collect and analyze your data can prevent them from impacting your work too much.
Receive feedback on language, structure, and formatting
Professional editors proofread and edit your paper by focusing on:
- Academic style
- Vague sentences
- Style consistency
See an example

Each of the research approaches involve using one or more data collection methods . These are some of the most common qualitative methods:
- Observations: recording what you have seen, heard, or encountered in detailed field notes.
- Interviews: personally asking people questions in one-on-one conversations.
- Focus groups: asking questions and generating discussion among a group of people.
- Surveys : distributing questionnaires with open-ended questions.
- Secondary research: collecting existing data in the form of texts, images, audio or video recordings, etc.
- You take field notes with observations and reflect on your own experiences of the company culture.
- You distribute open-ended surveys to employees across all the company’s offices by email to find out if the culture varies across locations.
- You conduct in-depth interviews with employees in your office to learn about their experiences and perspectives in greater detail.
Qualitative researchers often consider themselves “instruments” in research because all observations, interpretations and analyses are filtered through their own personal lens.
For this reason, when writing up your methodology for qualitative research, it’s important to reflect on your approach and to thoroughly explain the choices you made in collecting and analyzing the data.
Qualitative data can take the form of texts, photos, videos and audio. For example, you might be working with interview transcripts, survey responses, fieldnotes, or recordings from natural settings.
Most types of qualitative data analysis share the same five steps:
- Prepare and organize your data. This may mean transcribing interviews or typing up fieldnotes.
- Review and explore your data. Examine the data for patterns or repeated ideas that emerge.
- Develop a data coding system. Based on your initial ideas, establish a set of codes that you can apply to categorize your data.
- Assign codes to the data. For example, in qualitative survey analysis, this may mean going through each participant’s responses and tagging them with codes in a spreadsheet. As you go through your data, you can create new codes to add to your system if necessary.
- Identify recurring themes. Link codes together into cohesive, overarching themes.
There are several specific approaches to analyzing qualitative data. Although these methods share similar processes, they emphasize different concepts.
| Approach | When to use | Example |
|---|---|---|
| To describe and categorize common words, phrases, and ideas in qualitative data. | A market researcher could perform content analysis to find out what kind of language is used in descriptions of therapeutic apps. | |
| To identify and interpret patterns and themes in qualitative data. | A psychologist could apply thematic analysis to travel blogs to explore how tourism shapes self-identity. | |
| To examine the content, structure, and design of texts. | A media researcher could use textual analysis to understand how news coverage of celebrities has changed in the past decade. | |
| To study communication and how language is used to achieve effects in specific contexts. | A political scientist could use discourse analysis to study how politicians generate trust in election campaigns. |
Qualitative research often tries to preserve the voice and perspective of participants and can be adjusted as new research questions arise. Qualitative research is good for:
- Flexibility
The data collection and analysis process can be adapted as new ideas or patterns emerge. They are not rigidly decided beforehand.
- Natural settings
Data collection occurs in real-world contexts or in naturalistic ways.
- Meaningful insights
Detailed descriptions of people’s experiences, feelings and perceptions can be used in designing, testing or improving systems or products.
- Generation of new ideas
Open-ended responses mean that researchers can uncover novel problems or opportunities that they wouldn’t have thought of otherwise.
Here's why students love Scribbr's proofreading services
Discover proofreading & editing
Researchers must consider practical and theoretical limitations in analyzing and interpreting their data. Qualitative research suffers from:
- Unreliability
The real-world setting often makes qualitative research unreliable because of uncontrolled factors that affect the data.
- Subjectivity
Due to the researcher’s primary role in analyzing and interpreting data, qualitative research cannot be replicated . The researcher decides what is important and what is irrelevant in data analysis, so interpretations of the same data can vary greatly.
- Limited generalizability
Small samples are often used to gather detailed data about specific contexts. Despite rigorous analysis procedures, it is difficult to draw generalizable conclusions because the data may be biased and unrepresentative of the wider population .
- Labor-intensive
Although software can be used to manage and record large amounts of text, data analysis often has to be checked or performed manually.
If you want to know more about statistics , methodology , or research bias , make sure to check out some of our other articles with explanations and examples.
- Chi square goodness of fit test
- Degrees of freedom
- Null hypothesis
- Discourse analysis
- Control groups
- Mixed methods research
- Non-probability sampling
- Quantitative research
- Inclusion and exclusion criteria
Research bias
- Rosenthal effect
- Implicit bias
- Cognitive bias
- Selection bias
- Negativity bias
- Status quo bias
Quantitative research deals with numbers and statistics, while qualitative research deals with words and meanings.
Quantitative methods allow you to systematically measure variables and test hypotheses . Qualitative methods allow you to explore concepts and experiences in more detail.
There are five common approaches to qualitative research :
- Grounded theory involves collecting data in order to develop new theories.
- Ethnography involves immersing yourself in a group or organization to understand its culture.
- Narrative research involves interpreting stories to understand how people make sense of their experiences and perceptions.
- Phenomenological research involves investigating phenomena through people’s lived experiences.
- Action research links theory and practice in several cycles to drive innovative changes.
Data collection is the systematic process by which observations or measurements are gathered in research. It is used in many different contexts by academics, governments, businesses, and other organizations.
There are various approaches to qualitative data analysis , but they all share five steps in common:
- Prepare and organize your data.
- Review and explore your data.
- Develop a data coding system.
- Assign codes to the data.
- Identify recurring themes.
The specifics of each step depend on the focus of the analysis. Some common approaches include textual analysis , thematic analysis , and discourse analysis .
Cite this Scribbr article
If you want to cite this source, you can copy and paste the citation or click the “Cite this Scribbr article” button to automatically add the citation to our free Citation Generator.
Bhandari, P. (2023, June 22). What Is Qualitative Research? | Methods & Examples. Scribbr. Retrieved September 3, 2024, from https://www.scribbr.com/methodology/qualitative-research/
Is this article helpful?

Pritha Bhandari
Other students also liked, qualitative vs. quantitative research | differences, examples & methods, how to do thematic analysis | step-by-step guide & examples, "i thought ai proofreading was useless but..".
I've been using Scribbr for years now and I know it's a service that won't disappoint. It does a good job spotting mistakes”
- Privacy Policy
Home » Qualitative Research – Methods, Analysis Types and Guide
Qualitative Research – Methods, Analysis Types and Guide
Table of Contents

Qualitative Research
Qualitative research is a type of research methodology that focuses on exploring and understanding people’s beliefs, attitudes, behaviors, and experiences through the collection and analysis of non-numerical data. It seeks to answer research questions through the examination of subjective data, such as interviews, focus groups, observations, and textual analysis.
Qualitative research aims to uncover the meaning and significance of social phenomena, and it typically involves a more flexible and iterative approach to data collection and analysis compared to quantitative research. Qualitative research is often used in fields such as sociology, anthropology, psychology, and education.
Qualitative Research Methods

Qualitative Research Methods are as follows:
One-to-One Interview
This method involves conducting an interview with a single participant to gain a detailed understanding of their experiences, attitudes, and beliefs. One-to-one interviews can be conducted in-person, over the phone, or through video conferencing. The interviewer typically uses open-ended questions to encourage the participant to share their thoughts and feelings. One-to-one interviews are useful for gaining detailed insights into individual experiences.
Focus Groups
This method involves bringing together a group of people to discuss a specific topic in a structured setting. The focus group is led by a moderator who guides the discussion and encourages participants to share their thoughts and opinions. Focus groups are useful for generating ideas and insights, exploring social norms and attitudes, and understanding group dynamics.
Ethnographic Studies
This method involves immersing oneself in a culture or community to gain a deep understanding of its norms, beliefs, and practices. Ethnographic studies typically involve long-term fieldwork and observation, as well as interviews and document analysis. Ethnographic studies are useful for understanding the cultural context of social phenomena and for gaining a holistic understanding of complex social processes.
Text Analysis
This method involves analyzing written or spoken language to identify patterns and themes. Text analysis can be quantitative or qualitative. Qualitative text analysis involves close reading and interpretation of texts to identify recurring themes, concepts, and patterns. Text analysis is useful for understanding media messages, public discourse, and cultural trends.
This method involves an in-depth examination of a single person, group, or event to gain an understanding of complex phenomena. Case studies typically involve a combination of data collection methods, such as interviews, observations, and document analysis, to provide a comprehensive understanding of the case. Case studies are useful for exploring unique or rare cases, and for generating hypotheses for further research.
Process of Observation
This method involves systematically observing and recording behaviors and interactions in natural settings. The observer may take notes, use audio or video recordings, or use other methods to document what they see. Process of observation is useful for understanding social interactions, cultural practices, and the context in which behaviors occur.
Record Keeping
This method involves keeping detailed records of observations, interviews, and other data collected during the research process. Record keeping is essential for ensuring the accuracy and reliability of the data, and for providing a basis for analysis and interpretation.
This method involves collecting data from a large sample of participants through a structured questionnaire. Surveys can be conducted in person, over the phone, through mail, or online. Surveys are useful for collecting data on attitudes, beliefs, and behaviors, and for identifying patterns and trends in a population.
Qualitative data analysis is a process of turning unstructured data into meaningful insights. It involves extracting and organizing information from sources like interviews, focus groups, and surveys. The goal is to understand people’s attitudes, behaviors, and motivations
Qualitative Research Analysis Methods
Qualitative Research analysis methods involve a systematic approach to interpreting and making sense of the data collected in qualitative research. Here are some common qualitative data analysis methods:
Thematic Analysis
This method involves identifying patterns or themes in the data that are relevant to the research question. The researcher reviews the data, identifies keywords or phrases, and groups them into categories or themes. Thematic analysis is useful for identifying patterns across multiple data sources and for generating new insights into the research topic.
Content Analysis
This method involves analyzing the content of written or spoken language to identify key themes or concepts. Content analysis can be quantitative or qualitative. Qualitative content analysis involves close reading and interpretation of texts to identify recurring themes, concepts, and patterns. Content analysis is useful for identifying patterns in media messages, public discourse, and cultural trends.
Discourse Analysis
This method involves analyzing language to understand how it constructs meaning and shapes social interactions. Discourse analysis can involve a variety of methods, such as conversation analysis, critical discourse analysis, and narrative analysis. Discourse analysis is useful for understanding how language shapes social interactions, cultural norms, and power relationships.
Grounded Theory Analysis
This method involves developing a theory or explanation based on the data collected. Grounded theory analysis starts with the data and uses an iterative process of coding and analysis to identify patterns and themes in the data. The theory or explanation that emerges is grounded in the data, rather than preconceived hypotheses. Grounded theory analysis is useful for understanding complex social phenomena and for generating new theoretical insights.
Narrative Analysis
This method involves analyzing the stories or narratives that participants share to gain insights into their experiences, attitudes, and beliefs. Narrative analysis can involve a variety of methods, such as structural analysis, thematic analysis, and discourse analysis. Narrative analysis is useful for understanding how individuals construct their identities, make sense of their experiences, and communicate their values and beliefs.
Phenomenological Analysis
This method involves analyzing how individuals make sense of their experiences and the meanings they attach to them. Phenomenological analysis typically involves in-depth interviews with participants to explore their experiences in detail. Phenomenological analysis is useful for understanding subjective experiences and for developing a rich understanding of human consciousness.
Comparative Analysis
This method involves comparing and contrasting data across different cases or groups to identify similarities and differences. Comparative analysis can be used to identify patterns or themes that are common across multiple cases, as well as to identify unique or distinctive features of individual cases. Comparative analysis is useful for understanding how social phenomena vary across different contexts and groups.
Applications of Qualitative Research
Qualitative research has many applications across different fields and industries. Here are some examples of how qualitative research is used:
- Market Research: Qualitative research is often used in market research to understand consumer attitudes, behaviors, and preferences. Researchers conduct focus groups and one-on-one interviews with consumers to gather insights into their experiences and perceptions of products and services.
- Health Care: Qualitative research is used in health care to explore patient experiences and perspectives on health and illness. Researchers conduct in-depth interviews with patients and their families to gather information on their experiences with different health care providers and treatments.
- Education: Qualitative research is used in education to understand student experiences and to develop effective teaching strategies. Researchers conduct classroom observations and interviews with students and teachers to gather insights into classroom dynamics and instructional practices.
- Social Work : Qualitative research is used in social work to explore social problems and to develop interventions to address them. Researchers conduct in-depth interviews with individuals and families to understand their experiences with poverty, discrimination, and other social problems.
- Anthropology : Qualitative research is used in anthropology to understand different cultures and societies. Researchers conduct ethnographic studies and observe and interview members of different cultural groups to gain insights into their beliefs, practices, and social structures.
- Psychology : Qualitative research is used in psychology to understand human behavior and mental processes. Researchers conduct in-depth interviews with individuals to explore their thoughts, feelings, and experiences.
- Public Policy : Qualitative research is used in public policy to explore public attitudes and to inform policy decisions. Researchers conduct focus groups and one-on-one interviews with members of the public to gather insights into their perspectives on different policy issues.
How to Conduct Qualitative Research
Here are some general steps for conducting qualitative research:
- Identify your research question: Qualitative research starts with a research question or set of questions that you want to explore. This question should be focused and specific, but also broad enough to allow for exploration and discovery.
- Select your research design: There are different types of qualitative research designs, including ethnography, case study, grounded theory, and phenomenology. You should select a design that aligns with your research question and that will allow you to gather the data you need to answer your research question.
- Recruit participants: Once you have your research question and design, you need to recruit participants. The number of participants you need will depend on your research design and the scope of your research. You can recruit participants through advertisements, social media, or through personal networks.
- Collect data: There are different methods for collecting qualitative data, including interviews, focus groups, observation, and document analysis. You should select the method or methods that align with your research design and that will allow you to gather the data you need to answer your research question.
- Analyze data: Once you have collected your data, you need to analyze it. This involves reviewing your data, identifying patterns and themes, and developing codes to organize your data. You can use different software programs to help you analyze your data, or you can do it manually.
- Interpret data: Once you have analyzed your data, you need to interpret it. This involves making sense of the patterns and themes you have identified, and developing insights and conclusions that answer your research question. You should be guided by your research question and use your data to support your conclusions.
- Communicate results: Once you have interpreted your data, you need to communicate your results. This can be done through academic papers, presentations, or reports. You should be clear and concise in your communication, and use examples and quotes from your data to support your findings.
Examples of Qualitative Research
Here are some real-time examples of qualitative research:
- Customer Feedback: A company may conduct qualitative research to understand the feedback and experiences of its customers. This may involve conducting focus groups or one-on-one interviews with customers to gather insights into their attitudes, behaviors, and preferences.
- Healthcare : A healthcare provider may conduct qualitative research to explore patient experiences and perspectives on health and illness. This may involve conducting in-depth interviews with patients and their families to gather information on their experiences with different health care providers and treatments.
- Education : An educational institution may conduct qualitative research to understand student experiences and to develop effective teaching strategies. This may involve conducting classroom observations and interviews with students and teachers to gather insights into classroom dynamics and instructional practices.
- Social Work: A social worker may conduct qualitative research to explore social problems and to develop interventions to address them. This may involve conducting in-depth interviews with individuals and families to understand their experiences with poverty, discrimination, and other social problems.
- Anthropology : An anthropologist may conduct qualitative research to understand different cultures and societies. This may involve conducting ethnographic studies and observing and interviewing members of different cultural groups to gain insights into their beliefs, practices, and social structures.
- Psychology : A psychologist may conduct qualitative research to understand human behavior and mental processes. This may involve conducting in-depth interviews with individuals to explore their thoughts, feelings, and experiences.
- Public Policy: A government agency or non-profit organization may conduct qualitative research to explore public attitudes and to inform policy decisions. This may involve conducting focus groups and one-on-one interviews with members of the public to gather insights into their perspectives on different policy issues.
Purpose of Qualitative Research
The purpose of qualitative research is to explore and understand the subjective experiences, behaviors, and perspectives of individuals or groups in a particular context. Unlike quantitative research, which focuses on numerical data and statistical analysis, qualitative research aims to provide in-depth, descriptive information that can help researchers develop insights and theories about complex social phenomena.
Qualitative research can serve multiple purposes, including:
- Exploring new or emerging phenomena : Qualitative research can be useful for exploring new or emerging phenomena, such as new technologies or social trends. This type of research can help researchers develop a deeper understanding of these phenomena and identify potential areas for further study.
- Understanding complex social phenomena : Qualitative research can be useful for exploring complex social phenomena, such as cultural beliefs, social norms, or political processes. This type of research can help researchers develop a more nuanced understanding of these phenomena and identify factors that may influence them.
- Generating new theories or hypotheses: Qualitative research can be useful for generating new theories or hypotheses about social phenomena. By gathering rich, detailed data about individuals’ experiences and perspectives, researchers can develop insights that may challenge existing theories or lead to new lines of inquiry.
- Providing context for quantitative data: Qualitative research can be useful for providing context for quantitative data. By gathering qualitative data alongside quantitative data, researchers can develop a more complete understanding of complex social phenomena and identify potential explanations for quantitative findings.
When to use Qualitative Research
Here are some situations where qualitative research may be appropriate:
- Exploring a new area: If little is known about a particular topic, qualitative research can help to identify key issues, generate hypotheses, and develop new theories.
- Understanding complex phenomena: Qualitative research can be used to investigate complex social, cultural, or organizational phenomena that are difficult to measure quantitatively.
- Investigating subjective experiences: Qualitative research is particularly useful for investigating the subjective experiences of individuals or groups, such as their attitudes, beliefs, values, or emotions.
- Conducting formative research: Qualitative research can be used in the early stages of a research project to develop research questions, identify potential research participants, and refine research methods.
- Evaluating interventions or programs: Qualitative research can be used to evaluate the effectiveness of interventions or programs by collecting data on participants’ experiences, attitudes, and behaviors.
Characteristics of Qualitative Research
Qualitative research is characterized by several key features, including:
- Focus on subjective experience: Qualitative research is concerned with understanding the subjective experiences, beliefs, and perspectives of individuals or groups in a particular context. Researchers aim to explore the meanings that people attach to their experiences and to understand the social and cultural factors that shape these meanings.
- Use of open-ended questions: Qualitative research relies on open-ended questions that allow participants to provide detailed, in-depth responses. Researchers seek to elicit rich, descriptive data that can provide insights into participants’ experiences and perspectives.
- Sampling-based on purpose and diversity: Qualitative research often involves purposive sampling, in which participants are selected based on specific criteria related to the research question. Researchers may also seek to include participants with diverse experiences and perspectives to capture a range of viewpoints.
- Data collection through multiple methods: Qualitative research typically involves the use of multiple data collection methods, such as in-depth interviews, focus groups, and observation. This allows researchers to gather rich, detailed data from multiple sources, which can provide a more complete picture of participants’ experiences and perspectives.
- Inductive data analysis: Qualitative research relies on inductive data analysis, in which researchers develop theories and insights based on the data rather than testing pre-existing hypotheses. Researchers use coding and thematic analysis to identify patterns and themes in the data and to develop theories and explanations based on these patterns.
- Emphasis on researcher reflexivity: Qualitative research recognizes the importance of the researcher’s role in shaping the research process and outcomes. Researchers are encouraged to reflect on their own biases and assumptions and to be transparent about their role in the research process.
Advantages of Qualitative Research
Qualitative research offers several advantages over other research methods, including:
- Depth and detail: Qualitative research allows researchers to gather rich, detailed data that provides a deeper understanding of complex social phenomena. Through in-depth interviews, focus groups, and observation, researchers can gather detailed information about participants’ experiences and perspectives that may be missed by other research methods.
- Flexibility : Qualitative research is a flexible approach that allows researchers to adapt their methods to the research question and context. Researchers can adjust their research methods in real-time to gather more information or explore unexpected findings.
- Contextual understanding: Qualitative research is well-suited to exploring the social and cultural context in which individuals or groups are situated. Researchers can gather information about cultural norms, social structures, and historical events that may influence participants’ experiences and perspectives.
- Participant perspective : Qualitative research prioritizes the perspective of participants, allowing researchers to explore subjective experiences and understand the meanings that participants attach to their experiences.
- Theory development: Qualitative research can contribute to the development of new theories and insights about complex social phenomena. By gathering rich, detailed data and using inductive data analysis, researchers can develop new theories and explanations that may challenge existing understandings.
- Validity : Qualitative research can offer high validity by using multiple data collection methods, purposive and diverse sampling, and researcher reflexivity. This can help ensure that findings are credible and trustworthy.
Limitations of Qualitative Research
Qualitative research also has some limitations, including:
- Subjectivity : Qualitative research relies on the subjective interpretation of researchers, which can introduce bias into the research process. The researcher’s perspective, beliefs, and experiences can influence the way data is collected, analyzed, and interpreted.
- Limited generalizability: Qualitative research typically involves small, purposive samples that may not be representative of larger populations. This limits the generalizability of findings to other contexts or populations.
- Time-consuming: Qualitative research can be a time-consuming process, requiring significant resources for data collection, analysis, and interpretation.
- Resource-intensive: Qualitative research may require more resources than other research methods, including specialized training for researchers, specialized software for data analysis, and transcription services.
- Limited reliability: Qualitative research may be less reliable than quantitative research, as it relies on the subjective interpretation of researchers. This can make it difficult to replicate findings or compare results across different studies.
- Ethics and confidentiality: Qualitative research involves collecting sensitive information from participants, which raises ethical concerns about confidentiality and informed consent. Researchers must take care to protect the privacy and confidentiality of participants and obtain informed consent.
Also see Research Methods
About the author

Muhammad Hassan
Researcher, Academic Writer, Web developer
You may also like

Mixed Methods Research – Types & Analysis

Textual Analysis – Types, Examples and Guide

Descriptive Research Design – Types, Methods and...

Basic Research – Types, Methods and Examples

Survey Research – Types, Methods, Examples

Observational Research – Methods and Guide
What are the different types of qualitative research?
Last updated
8 February 2023
Reviewed by
Jean Kaluza
Short on time? Get an AI generated summary of this article instead
Qualitative research is a crucial step in product development . While the quantitative approach might explain where an issue lies and the number of users it affects, the qualitative method answers why the problem is happening and how it affects customers.
This type of research explains how people experience the world. Many researchers use it to understand a group’s behavior, characteristics, and motivations.
People also use qualitative research in the business sector. Qualitative research enables you to access content-rich information about user emotions and perceptions. For example, you can use it in market research to understand what a target group thinks about your company’s new ideas.
Different qualitative research types serve a particular purpose. Before we delve into the various types of qualitative research, let's begin with the basics.
Analyze all your qualitative research
Analyze qualitative data faster and surface more actionable insights
- What is qualitative research?
Qualitative research is a market research process that involves collecting and analyzing in-depth data through conversational and open-ended communication. It focuses on "what" people think and "why" they think so. Qualitative research goes beyond how many people do something to determine why they do or don't do it.
Qualitative research methods enable detailed questioning of respondents based on their responses. The researcher’s aim is to understand the participants’ feelings and motivations.
Imagine a cake company looking to get more customers at two branches on the same street. A systematic observation showed more people bought cakes from Branch A than from Branch B. One way to determine why people preferred Branch A is to interview potential customers.
Let's say the company visited both stores and interviewed customers. Upon completion, results showed that workers in Branch B lacked good customer relationships, so many people visited Branch A instead.
Another example is if marketing notices a consistent but unexplainable churn in customers. Maybe subscribers of the platform were only staying on for a month rather than a much longer expected timeline.
Qualitative initiatives could dive into the motivations of these users. Findings may reveal that the customers achieved their goals much faster than expected. Perhaps they didn’t have the characteristics the company originally assumed they had.
Qualitative research identifies customer pain points, determines why a particular product might not yield the desired results, and tests possible solutions. It’s a helpful tool when you’re looking to develop and improve products and services. Understanding how your audience makes decisions can help you draw valuable conclusions in market research.

Learn more about qualitative research platforms
- Characteristics of qualitative research methods
Qualitative research involves collecting and evaluating non-numerical data (audio, video, and text) to deeply understand opinions, concepts, or experiences. It also includes data about lived experiences, emotions, and behavior with the meaning people add to it.
Due to its softer manner, researchers express results more commonly in:
Video clips
Sound bites
Pull quotes
Here are the characteristics of qualitative research.
Real-time data
Qualitative research methods often collect data at the location where people encounter the product or company’s service. This ensures it’s as close to the authentic experience of its consumers as possible.
Many data sources
Qualitative researchers don't need to rely on a single source of data . They can gather different data types from sources like observations, interviews, and documents for better understanding.
Qualitative research techniques tend to break down complex problems into smaller, simpler pieces that focus on what the research intends to evaluate. The goal is to have a clear understanding of the unknown. That means you can uncover answers while leaving room for surprises and discoveries to emerge.
Raw information
Since qualitative research involves conversations, participants should be able to confide in the interviewer and give their honest opinions. Researchers should use qualitative interviewing techniques to establish trust and comfort in participants to facilitate authentic and pure reactions to products. That’s why you need to ensure the information you provide is accurate.
Free AI content analysis generator
Make sense of your research by automatically summarizing key takeaways through our free content analysis tool.

- Types of qualitative research methods with examples
Qualitative research methods reveal your target audiences' behavior and perception of a particular situation. Its results are more detailed and descriptive, so you can easily draw inferences from the data.
Each qualitative research type has its purpose and might not be suitable for all projects. Before conducting a qualitative study, it's crucial to understand the various types of qualitative research methods and how they differ.
Let's look at each of the six types of qualitative research methods.
1. Phenomenological method
The phenomenological approach explores the experiences of a specific phenomenon (observable fact or event) in a person or group. These are “lived experiences.”
The method helps researchers better understand people's beliefs, attitudes, behavior, and experiences. In this method, you ask customers to describe their experiences as they perceive them. This approach recognizes there is no single objective reality; everyone experiences things differently.
Researchers usually set their assumptions aside to remove bias (bracketing) and focus on the participants’ experiences.
While the outcome depends on the participants' points of view, researchers try to answer the following questions:
How do people experience this phenomenon?
How does it affect them?
What factors influence their experience?
This method uses information from interviews, observations, diary studies, or voice-of-customer sessions to determine a participant's feelings during a particular activity or event. During this research, it's vital to make your customers feel comfortable, so they share their honest experiences.
Your questions in phenomenological research should be free of closed-ended or leading questions. Closed-ended questions usually only require a simple one-word response and won’t tell the whole story or give you the actionable data you want to collect.
Leading questions require your user to contradict what your question may imply. This usually results in polite and natural agreement rather than the honest response you need. In short, don’t ask them if they like a feature. Ask your user how they feel about it, either positive or negative, and let them direct the discussion from there.
You can use this method to determine your customer's purchasing behavior. For example, you can ask questions like, "Do you prefer red velvet cake or vanilla cake? Why?" The responses will depend on their experiences. The result of this research method can be useful when you want to improve your product's quality or target a different product to increase sales.
2. Ethnographic model
This model is an in-depth observation that studies your target audience in their natural environment. It involves collecting and analyzing data about people by watching them rather than interviewing them. Quite often, consumers may report using a particular product in one way, but observing could prove otherwise.
It requires researchers to adapt to the environment of their target audience. Since it could be any location, collecting data can be challenging. But this model helps you understand the challenges, cultures, settings, and motivations that occur by seeing it yourself. With well-executed ethnographic research, your company can uncover:
Users' motivations behind using your product
How they’re using it
During what other activities are they using it
How they discovered it
And even why they stopped using it
All of these insights can help you build a more intuitive product experience that leaves consumers feeling heard and satisfied.
Companies that act on accurate ethnographic studies are often way ahead of their competitors since they have a clear idea of where their customers are and where they are going.
3. Grounded theory method
Sociologists Glaser and Strauss developed the grounded theory model in the 1960s. In this model, researchers collect, interpret, and analyze data to develop various theories regarding the research topic. Rather than establish theories before examining data, researchers develop theories after studying the data.
Researchers use this model in qualitative research to see what theories or questions arise from a given data set. They may group the drawn-out theories and analyze them further. Grounded theory needs careful content analysis since the emerging theories must be valid, else it can lead to lost insights and poor decision-making.
It is often a research method that builds on existing work. Data collection methods include interviews, observations, longitudinal studies , and diary studies.
4. Case study model
The case study model helps explain a particular element, family, person, business, or organization. It is common in fields like education and social sciences. Ways of collecting data in this model may include interviews since the research requires in-depth and real details. The researcher will ask questions to determine why a particular respondent acts the way they do.
For instance, a film streaming company might watch a family use their technology to determine their reaction to new services or products and what features could interest them.
5. Historical model
Historical studies involve identifying, locating, evaluating, and synthesizing data from the past. It doesn't only discover past events but tries to relate them to the present and future.
For instance, you can analyze data from previous advertising campaigns and use it to conduct a new one. Or a music management company can look at the audience from a 2022 concert to plan future ones.
Historical research requires great skill. Researchers must analyze the data, look for trends or changes, or pinpoint any contradictions. You can ask questions to design your research strategy, like, "How has consumer preference changed over the years?"
Sometimes, historical data can collect irrelevant data. Let’s consider how airlines experienced so much turmoil during the pandemic. It’s possible the historical data isn’t relevant enough to gather useful data from in a post-pandemic world.
6. Narrative model
The narrative method is one of the types of qualitative research methods that focuses on written and spoken words or visual representations by people. Here, stories become raw data.
Researchers evaluate people's lived experiences through questioning to determine issues they may face. This research method helps you understand what people think about your brand. You can use it to determine the various challenges your target audience faces on a personal narrative level.
- Qualitative research data collection
This is the process of obtaining information. Qualitative data collection involves obtaining non-numerical data. It provides researchers with detailed insights into why people make decisions. But to arrive at such conclusions, the collected data should be rich, holistic, and from participants that accurately represent your targeted audience.
Some ways to collect data in qualitative research include:
Participant observations
You collect data by watching other people's behavior closely and recording what you hear, see, or encounter.
One-on-one interviews
This involves an open-ended conversation with your target audience. The interview can be via phone, email, or face-to-face.
In-depth surveys
This may involve distributing a questionnaire with open-ended questions.
Focus groups
Here, a moderator asks participants (usually 6–12 members) predetermined questions about your products, brand, or services. It's crucial to avoid yes-or-no questions to promote engagement.
Voice-of-customer
Here, the moderator comes up with a feature or product concept and brainstorms the idea with a customer. The customer plays an active role in shaping the concept to ensure the feature really would be a solution for them.
Card-sorting
This method involves index cards with written content about a given service or product. The moderator asks the participant to think out loud while organizing cards in ways that make sense to the user.
Diary studies
Diary studies require users to keep a journal or diary of specific experiences and their thoughts around them. These studies typically take longer to complete the data-gathering stage.
Regardless of the method you use for collecting qualitative data, it will generate a large amount of data. For example, if a researcher uses one-on-one discussions or a focus group to collect data, there will be video recordings or written notes to analyze.

Diary study templates
- Qualitative research data analysis
Qualitative data analysis involves examining data to understand and derive meaning from it. It involves making notes, recording videos or audio, taking photos, or analyzing text documents.
Here are the steps involved in qualitative data analysis:
Prepare and organize your data: This could mean typing notes during sessions, including timestamps, or transcribing your audio.
Review and explore the data: Check the data for repeated patterns or ideas that emerge.
Create codes for the data and assign them : Develop a set of codes to separate your data into categories and assign them.
Spot recurring themes : Link codes together into overarching, cohesive themes.
Learn more about qualitative research data analysis software
- When to use qualitative research
Researchers use qualitative research methods to get factual data for in-depth insights. You can use qualitative research when you want to:
Develop a new product or generate an idea.
Understand the problem areas of your product or service thoroughly.
Improve your marketing strategy.
Understand your weaknesses and strengths according to your users.
Deeply explore potential consumers’ motivations, desires, and demographics to understand your company’s role within them.
Figure out how people perceive your brand, product, or services.
Stay well ahead of your competition by knowing your users better than they do.
Qualitative research helps brands understand the underlying motivations and reasons behind consumer behavior and decisions.
- Qualitative research methods vs. quantitative research methods
In a nutshell, qualitative research methods revolve around people's perspectives and their reasoning to solve the “why” and “how.” Quantitative research methods center on measurements and numbers to uncover what is happening and sometimes the timeline in which it happened.
Together, both research methods help companies get an accurate and in-depth insight into a situation. It’s important to understand their significant differences to know when to employ each.
Here is a table to help you understand how both research methods differ.
|
|
|
| Focuses on user motivations, “how” they do things, and "why" they think in that manner | Centers on the "what" and "when " of what happened in the data |
| Descriptive data | Numerical data |
| Holistic | Particularistic |
| Less-structured methods like focus groups, scripted in-depth interviews, participant observation, and case study | Structured methods like in-app data, surveys, and questionnaires |
| More personal and direct contact with participants | Less personal and direct contact with participants |
| Open-ended | Close-ended |
| User responses can influence what question the researcher will ask next | User responses don't usually affect what question the researcher asks next |
| Why do you prefer green apples? | Did you buy a green apple today? A. Yes B. No |
What is the most common type of qualitative research?
A detailed interview is the most common type of qualitative research approach.
What is the most common form of qualitative interviewing?
A semi-structured interview is the most common form of qualitative interviewing. User testing is considered a qualitative interview in a one-on-one live environment.
What is the most common method used for qualitative data analysis?
Pattern matching is one of the commonest methods used for qualitative data analysis. Pattern matching involves forming a mental model to categorize all collected data into compartments to compare and evaluate.
Should you be using a customer insights hub?
Do you want to discover previous research faster?
Do you share your research findings with others?
Do you analyze research data?
Start for free today, add your research, and get to key insights faster
Editor’s picks
Last updated: 18 April 2023
Last updated: 27 February 2023
Last updated: 22 August 2024
Last updated: 5 February 2023
Last updated: 16 August 2024
Last updated: 9 March 2023
Last updated: 30 April 2024
Last updated: 12 December 2023
Last updated: 11 March 2024
Last updated: 4 July 2024
Last updated: 6 March 2024
Last updated: 5 March 2024
Last updated: 13 May 2024
Latest articles
Related topics, .css-je19u9{-webkit-align-items:flex-end;-webkit-box-align:flex-end;-ms-flex-align:flex-end;align-items:flex-end;display:-webkit-box;display:-webkit-flex;display:-ms-flexbox;display:flex;-webkit-flex-direction:row;-ms-flex-direction:row;flex-direction:row;-webkit-box-flex-wrap:wrap;-webkit-flex-wrap:wrap;-ms-flex-wrap:wrap;flex-wrap:wrap;-webkit-box-pack:center;-ms-flex-pack:center;-webkit-justify-content:center;justify-content:center;row-gap:0;text-align:center;max-width:671px;}@media (max-width: 1079px){.css-je19u9{max-width:400px;}.css-je19u9>span{white-space:pre;}}@media (max-width: 799px){.css-je19u9{max-width:400px;}.css-je19u9>span{white-space:pre;}} decide what to .css-1kiodld{max-height:56px;display:-webkit-box;display:-webkit-flex;display:-ms-flexbox;display:flex;-webkit-align-items:center;-webkit-box-align:center;-ms-flex-align:center;align-items:center;}@media (max-width: 1079px){.css-1kiodld{display:none;}} build next, decide what to build next, log in or sign up.
Get started for free
Extract insights from Customer & Employee Interviews. At Scale.
Explore top qualitative research types and examples.
Home » Explore top qualitative research types and examples
Qualitative research types offer rich insights into human behaviors, motivations, and experiences. In exploring these methodologies, researchers can uncover nuanced perspectives that quantitative approaches may overlook. This section delves into various qualitative research types, illustrating their distinctive characteristics and applications.
By understanding these research types, stakeholders can select the most suitable methods for their objectives. From in-depth interviews to focus groups, each type serves a unique purpose in gathering data. This nuanced understanding not only enhances the research quality but also informs decision-making processes across various sectors.
Top Qualitative Research Types
Qualitative research types provide valuable insights through a variety of methods focused on understanding human behavior, emotions, and experiences. Among the most popular types are interviews, focus groups, ethnography, and case studies. Each method offers unique advantages in collecting data that reflects the subjective perspectives of participants.
In-depth interviews allow researchers to explore personal experiences and motivations, yielding rich qualitative data. Focus groups facilitate dynamic discussions and highlight collective opinions or trends among participants. Ethnography immerses researchers in the participants' environments, often revealing how context influences behavior. Finally, case studies focus on a specific instance or population, helping to gather detailed information that can inform broader conclusions. Understanding these qualitative research types is crucial for anyone looking to gain deeper insights into human behavior and societal trends.
Ethnography: Exploring Cultural Phenomena
Ethnography serves as a vital qualitative research type, delving deep into cultural phenomena. By immersing researchers in specific communities, it unveils the subtleties of social interactions and behaviors. This form of research not only captures the lived experiences of individuals but also highlights the broader cultural narratives at play. Ethnographers may conduct interviews, observe daily activities, and participate in community events, providing striking insights into cultural values and practices.
This method enriches our understanding of human experiences by revealing trends that survey data may overlook. It empowers researchers to explore topics such as identity, tradition, and social structures in authentic contexts. Ethnography, therefore, plays an essential role in qualitative research types, making it a powerful tool for uncovering the complexities of cultural dynamics. By appreciating these nuances, we can foster a deeper understanding of society and its diverse practices.
Phenomenology: Understanding Human Experiences
Phenomenology focuses on understanding human experiences by exploring how individuals perceive and make sense of their worlds. In qualitative research types, it emphasizes lived experiences, allowing researchers to delve deeply into individuals' subjective realities. This approach seeks to gather rich, detailed descriptions of experiences and identify common themes that resonate within these narratives.
When employing phenomenology, researchers often conduct in-depth interviews, facilitating open-ended conversations that encourage participants to share their feelings and thoughts. By analyzing these narratives, researchers can uncover underlying meanings and insights about specific phenomena. This qualitative research type not only enhances comprehension but also fosters empathy towards diverse human experiences, making it invaluable in fields like psychology, healthcare, and education. Through this approach, phenomenology enriches qualitative research, clarifying the complexities of human existence and behavior.
Examples of Qualitative Research Types in Practice
Qualitative research types are widely used to better understand people's experiences, behaviors, and emotions. One prominent method is in-depth interviews, where researchers engage participants in one-on-one discussions to gather rich, detailed insights. This approach allows the researcher to explore participants' feelings and motivations behind their actions, providing a deeper context than quantitative data alone.
Another common practice is focus groups, which facilitate dynamic discussions among a small group of individuals. This setting encourages participants to share ideas and opinions, often leading to revelations about group dynamics and collective preferences. Observational studies also play a crucial role; researchers directly observe subjects in natural settings to capture authentic behavior. These qualitative research types collectively enhance understanding of complex social phenomena, making them invaluable tools for exploring nuanced human experiences.
Ethnographic Study: Observing Social Interactions
Ethnographic study involves immersive research methods aimed at understanding social interactions within specific cultures or communities. Researchers typically observe participants in their natural environments, noting behaviors, rituals, and social dynamics over time. This approach helps uncover nuanced insights that quantitative methods might overlook.
One key element involves participant observation, where researchers engage with subjects to gain deeper insights into their experiences and perspectives. Another crucial aspect is in-depth interviews, allowing researchers to capture personal narratives and contextual stories that enrich the data. Moreover, annotating environmental factors, like the setting and community dynamics, enables a comprehensive understanding of social interactions. Ultimately, through these qualitative research types, ethnographic studies reveal complex layers of meaning within social contexts, offering invaluable insights for various fields, including anthropology, sociology, and market research.
Phenomenological Study: Investigating Lived Experiences
Phenomenological studies focus on exploring the lived experiences of individuals, aiming to understand how they interpret their reality. This qualitative research type is grounded in the belief that personal experiences shape human perception and understanding. By engaging with participants through in-depth interviews, researchers can delve into the subjective meanings assigned to different experiences, such as health challenges, educational journeys, or traumatic events.
The process involves multiple steps, including selecting participants, designing open-ended questions, and analyzing responses for thematic patterns. Each participant's unique perspective contributes to the richness of the data collected. This method enables researchers to gain profound insights into how individuals navigate and make sense of their world, ultimately informing broader implications for practices, policies, and community understanding. Through such interpretations, phenomenological studies illuminate the essence of human experiences, contributing significantly to qualitative research types.
Conclusion: The Importance of Qualitative Research Types
Qualitative research types play a pivotal role in understanding human behavior, emotions, and reactions. By embracing methods such as interviews, focus groups, and observations, researchers can gather deep insights that are often overlooked in quantitative studies. These qualitative insights aid in uncovering motivations and pain points, leading to more targeted solutions for real-world problems.
Moreover, the diversity of qualitative research approaches allows for a comprehensive view of complex issues. This breadth enables researchers to adapt their methods to suit specific contexts, ensuring that the data collected is both relevant and actionable. In conclusion, qualitative research types are indispensable for obtaining meaningful insights that foster innovation and improve decision-making across various fields.
Turn interviews into actionable insights
On this Page
How to apply psychographics segmentation examples in marketing
You may also like, guide to designing a website user journey map.

7 Usability Testing Methods to Improve User Experience
Top 5 free ux research tools to use in 2024.
Unlock Insights from Interviews 10x faster
- Request demo
- Get started for free
- Open access
- Published: 02 September 2024
“I am there just to get on with it”: a qualitative study on the labour of the patient and public involvement workforce
- Stan Papoulias ORCID: orcid.org/0000-0002-7891-0923 1 &
- Louca-Mai Brady 2
Health Research Policy and Systems volume 22 , Article number: 118 ( 2024 ) Cite this article
18 Altmetric
Metrics details
Workers tasked with specific responsibilities around patient and public involvement (PPI) are now routinely part of the organizational landscape for applied health research in the United Kingdom. Even as the National Institute for Health and Care Research (NIHR) has had a pioneering role in developing a robust PPI infrastructure for publicly funded health research in the United Kingdom, considerable barriers remain to embedding substantive and sustainable public input in the design and delivery of research. Notably, researchers and clinicians report a tension between funders’ orientation towards deliverables and the resources and labour required to embed public involvement in research. These and other tensions require further investigation.
This was a qualitative study with participatory elements. Using purposive and snowball sampling and attending to regional and institutional diversity, we conducted 21 semi-structured interviews with individuals holding NIHR-funded formal PPI roles across England. Interviews were analysed through reflexive thematic analysis with coding and framing presented and adjusted through two workshops with study participants.
We generated five overarching themes which signal a growing tension between expectations put on staff in PPI roles and the structural limitations of these roles: (i) the instability of support; (ii) the production of invisible labour; (iii) PPI work as more than a job; (iv) accountability without control; and (v) delivering change without changing.
Conclusions
The NIHR PPI workforce has enabled considerable progress in embedding patient and public input in research activities. However, the role has led not to a resolution of the tension between performance management priorities and the labour of PPI, but rather to its displacement and – potentially – its intensification. We suggest that the expectation to “deliver” PPI hinges on a paradoxical demand to deliver a transformational intervention that is fundamentally divorced from any labour of transformation. We conclude that ongoing efforts to transform health research ecologies so as to better respond to the needs of patients will need to grapple with the force and consequences of this paradoxical demand.
Peer Review reports
Introduction – the labour of PPI
The inclusion of patients, service users and members of the public in the design, delivery and governance of health research is increasingly embedded in policy internationally, as partnerships with the beneficiaries of health research are seen to increase its relevance, acceptability and implementability. In this context, a growing number of studies have sought to evaluate the impact of public participation on research, including identifying the barriers and facilitators of good practice [ 1 , 2 , 3 , 4 , 5 , 6 , 7 , 8 ]. Some of this inquiry has centred on power, control and agency. Attention has been drawn, for example, to the scarcity of user or community-led research and to the low status of experiential knowledge in the hierarchies of knowledge production guiding evidence-based medicine [ 9 ]. Such hierarchies, authors have argued, constrain the legitimacy that the experiential knowledge of patients can achieve within academic-led research [ 10 ], may block the possibility of equitable partnerships such as those envisioned in co-production [ 11 ] and may function as a pull back against more participatory or emancipatory models of research [ 12 , 13 , 14 ]. In this way, patient and public inclusion in research may become less likely to aim towards inclusion of public and patient-led priorities, acting instead as kind of a “handmaiden” to research, servicing and validating institutionally pre-defined research goals [ 15 , 16 , 17 ].
Research on how public participation-related activities function as a form of labour within a research ecosystem, however, is scarce [ 18 ]. In this paper, we examine the labour of embedding such participation, with the aim of understanding how such labour fits within the regimes of performance management underpinning current research systems. We argue that considering this “fit” is crucial for a broader understanding of the implementation of public participation and therefore its potential impact on research delivery. To this end, we present findings from a UK study of the labour of an emerging professional cadre: “patient and public involvement” leads, managers and co-ordinators (henceforth PPI, the term routinely used for public participation in the United Kingdom). We concentrate specifically on staff working on research partnerships and centres funded by the National Institute for Health and Care Research (NIHR). This focus on the NIHR is motivated by the organization’s status as the centralized research and development arm of the National Health Service (NHS), with an important role in shaping health research systems in the United Kingdom since 2006. NIHR explicitly installed PPI in research as a foundational part of its mission and is currently considered a global leader in the field [ 19 ]. We contend that exploring the labour of this radically under-investigated workforce is crucial for understanding what we see as the shifting tensions – outlined in later sections – that underpin the key policy priority of embedding patients as collaborators in applied health research. To contextualize our study, we first consider how the requirement for PPI in research relates to the overall policy rationale underpinning the organizational mission of the NIHR as the NHS’s research arm, then consider existing research on tensions identified in efforts to embed PPI in a health system governed through regimes of performance management and finally articulate the ways in which dedicated PPI workers’ responsibilities have been developed as a way to address these tensions.
The NIHR as a site of “reformed managerialism”
The NIHR was founded in 2006 with the aim of centralizing and rationalizing NHS research and development activities. Its foundation instantiated the then Labour government’s efforts to strengthen and consolidate health research in the UK while also tackling some of the problems associated with the earlier introduction of new public management (NPM) principles in the governance of public services. NPM had been introduced in the UK public sector by Margaret Thatcher’s government, in line with similar trends in much of the Global North [ 20 ]. The aim was to curb what the Conservatives saw as saw as excesses in both public spending and professional autonomy. NPM consisted in management techniques adapted from the private sector: in the NHS this introduction was formalized via the 1990 National Health Service and Community Care Act, which created an internal market for services, with local authorities purchasing services from local health providers (NHS Trusts) [ 21 ]; top-down management control; an emphasis on cost-efficiency; a focus on targets and outputs over process; an intensification of metrics for performance management; and a positioning of patients and the public as consumers of health services with a right to choose [ 22 , 23 ]. In the context of the NHS, cost-efficiency meant concentrating on services and on research which would have the greatest positive impact on population health while preventing research waste [ 24 ]. By the mid-1990s, however, considerable criticism had been directed towards this model, including concerns that NPM techniques resulted in silo-like operations and public sector fragmentation, which limited the capacity for collaboration between services essential for effective policy. Importantly, there was also a sense that an excessive managerialism had resulted in a disconnection of public services from public and civic aims, that is, from the values, voices and interests of the public [ 25 , 26 ].
In this context, the emergence of the NIHR can be contextualized through the succeeding Labour government’s much publicized reformed managerialism, announced in their 1997 white paper “The New NHS: Modern, Dependable” [ 27 ]. Here, the reworking of NPM towards “network governance” meant that the silo-like effects of competition and marketization were to be attenuated through a turn to cross-sector partnerships and a renewed attention to quality standards and to patients’ voices [ 28 ]. It has been argued, however, that the new emphasis on partnerships did not undermine the dominance of performance management, while the investment in national standards for quality and safety resulted in an intensified metricization, with the result that this reform may have been more apparent than real, amounting to “NPM with a human face” [ 29 , 30 , 31 ]. Indeed, the NIHR can be seen as an exemplary instantiation of this model: as a centralized commissioner of research for the NHS, the NIHR put in place reporting mechanisms and performance indicators to ensure transparent and cost-efficient use of funds, with outputs and impact measured, managed and ranked [ 24 ]. At the same time, the founding document of the NIHR, Best Research for Best Health, articulates the redirection of such market-oriented principles towards a horizon of public good and patient benefit. The document firmly and explicitly positioned patients and the public as both primary beneficiaries of and important partners in the delivery of health research. People (patients) were to be placed “at the centre of a research system that focuses on quality, transparency and value for money” [ 32 ], a mission implemented through the installation of “structures and mechanisms to facilitate increased involvement of patients and the public in all stages of NHS Research & Development” [ 33 ]. This involvement would be supported by the advisory group INVOLVE, a key part of the new centralized health research system. INVOLVE, which had started life in 1996 as Consumers in NHS Research, funded by the Department of Health, testified to the Labour administration’s investment in championing “consumer” involvement in NHS research as a means of increasing research relevance [ 34 ]. The foundation of the NIHR then exemplified the beneficent alignment of NPM with public benefit, represented through the imaginary of a patient-centred NHS, performing accountability to the consumers/taxpayers through embedding PPI in all its activities. In this context, “public involvement” functioned as the lynchpin through which such alignment could be effected.
PPI work and the “logic of deliverables”: a site of tension
Existing research on the challenges of embedding PPI has typically focussed on the experiences of academics tasked with doing so within university research processes. For example, Pollard and Evans, in a 2013 paper, argue that undertaking PPI work in mental health research can be arduous, emotionally taxing and time consuming, and as such, can be in tension with expectations for cost-efficient and streamlined delivery of research outputs [ 35 ]. Similarly, Papoulias and Callard found that the “logic of deliverables” governing research funding can militate against undertaking PPI or even constitute PPI as “out of sync” with research timelines [ 36 ]. While recent years have seen a deepening operationalization of PPI in the NIHR and beyond, there are indications that this process, rather than removing these tensions, may have recast them in a different form. For example, when PPI is itself set up as performance-based obligation, researchers, faced with the requirement to satisfy an increasing number of such obligations, may either engage in “surface-level spectacles” to impress the funder while eschewing the long-term commitment necessary for substantive and ongoing PPI, or altogether refuse to undertake PPI, relegating the responsibility to others [ 37 , 38 ]. Such refusals may then contribute to a sharpening of workplace inequalities: insofar as PPI work is seen as “low priority” for more established academic staff, it can be unevenly distributed within research organizations, with precariously employed junior researchers and women typically assigned PPI responsibilities with the assumption that they possess the “soft skills” necessary for these roles [ 39 ].
Notably, the emergence of a dedicated PPI workforce is intended as a remedy for this tension by providing support, expertise and ways of negotiating the challenges associated with undertaking PPI responsibilities. In the NIHR, this workforce is part of a burgeoning infrastructure for public involvement which includes national standards, training programmes, payment guidelines, reporting frameworks and impact assessments [ 40 , 41 , 42 , 43 , 44 , 45 ]. By 2015, an INVOLVE review of PPI activities during the first 10 years of the NIHR attested to “a frenzy of involvement activity…across the system”, including more than 200 staff in PPI-related roles [ 40 ]. As NIHR expectations regarding PPI have become more extensive, responsibilities of PPI workers have proliferated, with INVOLVE organizing surveys and national workshops to identify their skills and support needs [ 41 , 42 ]. In 2019, the NIHR mandated the inclusion of a “designated PPI lead” in all funding applications, listing an extensive and complex roster of responsibilities. These now included delivery and implementation of long-term institutional strategies and objectives, thus testifying to the assimilation of involvement activities within the roster of “performance-based obligations” within research delivery systems [ 43 ]. Notably however, this formalization of PPI responsibilities is ambiguous: the website states that the role “should be a budgeted and resourced team member” and that they should have “the relevant skills, experience and authority”, but it does not specify whether this should be a researcher with skills in undertaking PPI or indeed someone hired specifically for their skills in PPI, that is, a member of the PPI workforce. Equally, the specifications, skills and support needs, which have been brought together into a distinct role, have yet to crystallize into a distinct career trajectory.
Case studies and evaluations of PPI practice often reference the skills and expertise required in leading and managing PPI. Chief among them are relational and communication skills: PPI workers have been described as “brokers” who mediate and enable learning between research and lay spaces [ 44 , 45 ]; skilled facilitators enabling inclusive practice [ 46 , 47 , 48 ]; “boundary spanners” navigating the complexities of bridging researchers with public contributors and undertaking community engagement through ongoing relational work [ 49 ]. While enumerating the skillset required for PPI work, some of these studies have identified a broader organizational devaluation of PPI workers: Brady and colleagues write of PPI roles as typically underfunded with poor job security, which undermines the continuity necessary for generating trust in PPI work [ 46 ], while Mathie and colleagues report that many PPI workers describe their work as “invisible”, a term which the authors relate to the sociological work on women’s labour (particularly housework and care labour) which is unpaid and rendered invisible insofar as it is naturalized as “care” [ 50 ]. Research on the neighbouring role of public engagement professionals in UK universities, which has been more extensive than that on PPI roles, can be instructive in fleshing out some of these points: public engagement professionals (PEPs) are tasked with mediating between academics and various publics in the service of a publicly accountable university. In a series of papers on the status of PEPs in university workplaces, Watermeyer and colleagues argue that, since public engagement labour is relegated to non-academic forms of expertise which lack recognition, PEPs’ efforts in boundary spanning do not confer prestige. This lack of prestige can, in effect, function as a “boundary block” obstructing PEPs’ work [ 51 , 52 ]. Furthermore, like Mathie and Brady, Watermeyer and colleagues also argue that the relational and facilitative nature of engagement labour constitutes such labour as feminized and devalued, with PEPs also reporting that their work remains invisible to colleagues and institutional audit instruments alike [ 50 , 53 ].
The present study seeks to explore further these suggestions that PPI labour, like that of public engagement professionals, lacks recognition and is constituted as invisible. However, we maintain that there are significant differences between the purpose and moral implications of involvement and engagement activities. PPI constitutes an amplification of the moral underpinnings of engagement policies: while public engagement seeks to showcase the public utility of academic research, public involvement aims to directly contribute to optimizing and personalizing healthcare provision by minimizing research waste, ensuring that treatments and services tap into the needs of patient groups, and delivering the vision of a patient-centred NHS. Therefore, even as PPI work may be peripheral to other auditable research activities, it is nevertheless central to the current rationale for publicly funded research ecosystems: by suturing performance management and efficiency metrics onto a discourse of public benefit, such work constitutes the moral underpinnings of performance management in health research systems. Therefore, an analysis of the labour of the dedicated PPI workforce is crucial for understanding how this suturing of performance management and “public benefit” works over the conjured figures of patients in need of benefit. This issue lies at the heart of our research study.
Our interview study formed the first phase of a multi-method qualitative inquiry into the working practices of NIHR-funded PPI leads. While PPI lead posts are in evidence in most NIHR-funded research, we decided to focus on NIHR infrastructure funding specifically: these are 5-year grants absorbing a major tranche of NIHR funds (over £600 million annually in 2024). They function as “strategic investments” embodying the principles outlined in Best Research for Best Health: they are awarded to research organizations and NHS Trusts for the purposes of developing and consolidating capacious environments for early stage and applied clinical research, including building a research delivery workforce and embedding a regional infrastructure of partnerships with industry, the third sector and patients and communities [ 55 ]. We believe that understanding the experience of the PPI workforce funded by these grants may give better insights into NIHR’s ecosystem and priorities, since they are specifically set up to support the development of sustainable partnerships and embed the translational pipeline into clinical practice.
The study used purposive sampling with snowball elements. In 2020–2021, we mapped all 72 NIHR infrastructure grants, identified the PPI teams working in each of these using publicly available information (found on the NIHR website and the websites and PPI pages of every organization awarded infrastructure grants) and sent out invitation emails to all teams. Where applicable, we also sent invitations to mailing lists of PPI-lead national networks connected to these grants. Inclusion criteria were that potential participants should have oversight roles, and/or be tasked with cross-programme/centre responsibilities, meaning that their facilitative and strategy building roles should cover the entirety of activities funded by one (and sometimes more than one) NIHR infrastructure grant or centres including advisory roles over most or all research projects associated with the centre of grant, and that they had worked in this or a comparable environment for 2 years.
The individuals who showed interest received detailed information sheets. Once they agreed to participate, they were sent a consent form and a convenient interview time was agreed. We conducted 21 semi-structured interviews online, between March and June 2021, lasting 60–90 min. The interview topic guide was developed in part through a review of organizational documents outlining the role and through a consideration of existing research on the labour of PPI within health research environments. It focussed on how PPI workers fit within the organization relationship between the actual work undertaken and the way this work is represented to both the organization and the funder. Interview questions included how participants understand their role; how they fit in the organization; how their actual work relates to the job description; how their work is understood by both colleagues and public contributors; the relationship between the work they undertake and how this is represented in reports to funder and presentations; and what they find challenging about their work. Information about participants’ background and what brought them to their present role was also gathered. Audio files were checked, transcribed and the transcripts fully de-identified. All participants were given the opportunity to check transcripts and withdraw them at any point until December 2021. None withdrew.
We analysed the interviews using reflexive thematic analysis with participatory elements [ 54 , 55 ]. Reflexive thematic analysis emphasizes the interpretative aspects of the analytical process, including the data “collection” process itself, which this approach recognizes as a generative act, where meaning is co-created between interviewer and participant and the discussion may be guided by the participant rather than strictly adhering to the topic guide [ 56 ]. We identified patterns of meaning through sustained and immersive engagement with the data. NVivo 12 was used for coding, while additional notes and memos on the Word documents themselves mitigated the over-fragmentation that might potentially limit NVivo as a tool for qualitative analysis. Once we had developed themes which gave a thorough interpretation of the data, we presented these to participants in two separate workshops to test for credibility and ensure that participants felt ownership of the process [ 57 ].
As the population from which the sample was taken is quite small, with some teams working across different infrastructure grants, confidentiality and anonymity were important concerns for participants. We therefore decided neither to collect nor to present extensive demographic information to preserve confidentiality and avoid deductive disclosure [ 58 ]. Out of our 21 participants 20 were women; there was some diversity in age, ethnicity and heritage, with a significant majority identifying as white (British or other European). Participants had diverse employment histories: many had come from other university or NHS posts, often in communications, programme management or human resources; a significant minority had come from the voluntary sector; and a small minority from the private sector. As there was no accredited qualification in PPI at the time this study was undertaken, participants had all learned their skills on their present or previous jobs. A total of 13 participants were on full-time contracts, although in several cases funding for these posts was finite and fragmented, often coming from different budgets.
In this paper we present five inter-related themes drawing on the conceptual architecture we outlined in the first half of this paper to explore how PPI workers navigate a research ecosystem of interlocking institutional spaces that is governed by “NPM with a human face”, while striving to align patients and the public with the imaginary of the patient-centred NHS that mobilizes the NIHR mission. These five themes are: (i) the instability of support; (ii) the production of invisible labour; (iii) PPI as moral imperative; (iv) accountability without control; and (v) delivering change without changing.
“There to grease the cogs rather than be the cogs”: the instability of “support”
Infrastructure grants act as a hub for large numbers of studies, often in diverse health fields, most of which should, ideally, include PPI activities. Here, dedicated PPI staff typically fulfil a cross-cutting role: they are meant to oversee, provide training and advise on embedding PPI activities across the grant and, in so doing, support researchers in undertaking PPI. On paper, support towards the institution in the form of training, delivering strategy for and evaluating PPI is associated with more senior roles (designated manager or lead) whereas support towards so-called public contributors is the remit of more junior roles (designated co-ordinator or officer) and can include doing outreach, facilitating, attending to access needs and developing payment and compensation procedures. However, these distinctions rarely applied in practice: participants typically reported that their work did not neatly fit into these categories and that they often had to fulfil both roles regardless of their title. Some were the only person in the team specifically tasked with PPI, and so their “lead” or “manager” designation was more symbolic than actual:
I have no person to manage, although sometimes I do get a little bit of admin support, but I don’t have any line management responsibility. It is really about managing my workload, working with people and managing the volunteers that I work with and administrating those groups and supporting them (P11).
P11’s title was manager but, as they essentially worked alone, shuttling between junior and senior role responsibilities, they justified and made sense of their title by reframing their support work with public contributors as “management”. Furthermore, other participants reported that researchers often misunderstood PPI workers’ cross-cutting role and expected them to both advise on and deliver PPI activities themselves, even in the context of multiple projects, thus altogether releasing researchers of such responsibility.
As a PPI lead, it is very difficult to define what your role is in different projects….and tasks … So, for example, I would imagine in [some cases] we are seen as the go-to if they have questions. [..] whereas, in [other cases], it is like, “Well, that’s your job because you’re the PPI lead” […] there is not a real understanding that PPI is everyone’s responsibility and that the theme leads are there to facilitate and to grease the cogs rather than be the cogs (P20).
Furthermore, participants reported that the NIHR requirement for a PPI lead in all funding applications might in fact have facilitated this slippage. As already mentioned, the NIHR requirement does not differentiate between someone hired specifically to undertake PPI and a researcher tasked with PPI activities. The presence of a member of staff with a “PPI lead” title thus meant that PPI responsibilities in individual research studies could continue to accrue on that worker:
The people who have been left with the burden of implementing [the NIHR specified PPI lead role] are almost exclusively people like me, though, because now researchers expect me to allow myself to be listed on their project as the PPI lead, and I actually wrote a document about what they can do for the PPI lead that more or less says, “Please don’t list me as your PPI lead. Please put aside funds to buy a PPI lead and I will train them, because there is only one me; I can’t be the PPI lead for everyone” (P10).
This expectation that core members of staff with responsibilities for PPI would also be able to act as PPI leads for numerous research projects suggests that this role lacks firm organizational co-ordinates and boundaries. Here, the presence of a PPI workforce does not, in fact, constitute an appropriate allocation of PPI labour but rather testifies to a continuing institutional misapprehension of the nature of such labour particularly in terms of its duration, location and value.
Conjuring PPI: the production of invisible labour
Participants consistently emphasized the invisibility of the kinds of labour, both administrative and relational, specific to public involvement as a process, confirming the findings of Mathie and colleagues [ 50 ]. This invisibility took different forms and had different justifications. Some argued that key aspects of their work, which are foundational to involvement, such as the process of relationship building, do not lend themselves to recognition as a performance indicator: “ There is absolutely no measure for that because how long is a piece of string” (P11). In addition, relationship building necessitated a considerably greater time investment than was institutionally acceptable, and this was particularly evident when it came to outreach. Participants who did their work in community spaces told stories of uncomprehending line-managers, or annoyed colleagues who wondered where the PPI worker goes and what they do all day:
There is very little understanding from colleagues about what I do on a day-to-day basis, and it has led to considerable conflict …. I would arrive at the office and then I would be disappearing quite promptly out into the community, because that is where I belong […] So, it is actually quite easy to become an absent person (P3).
Once again, the NIHR requirement for designated PPI leads in funding applications, intended to raise the visibility of PPI work by formalizing it as costed labour, could instead further consolidate its invisibility:
I am constantly shoved onto bids as 2% of my full-time equivalent and I think I worked out for a year that would be about 39 hours a year. For a researcher, popping the statistician down and all these different people on that bid, “Everyone is 2% and we need the money to run the trial, so 2% is fine”. And if I said to them, “Well, what do you think I would do in those 39 hours?” they wouldn’t have a clue, not a clue (P17).
The 2% of a full-time allocation is accorded to the PPI worker because 2–5% is the time typically costed for leadership roles or for roles with a circumscribed remit (e.g. statisticians). However, this allocation, in making PPI workers’ labour visible either as oversight (what project leads do) or as methodological expertise (what statisticians do), ends up producing the wrong kind of visibility: the 39 h mentioned here might make sense when the role mainly involves chairing weekly meetings or delivering statistical models but are in no way sufficient for the intense and ongoing labour of trust-building and alignment between institutions and public contributors in PPI.
Indeed, such costings, by eliding the complexity and duration of involvement, may reinforce expectations that PPI can be simply conjured up at will and delivered on demand:
A researcher will say to us, “I would really like you to help me to find some people with lived experience, run a focus group and then I’ll be away”. To them, that is the half-hour meeting to talk about this request, maybe 10 minutes to draft a tweet and an email to a charity that represents people with that condition […] the reality is it is astronomically more than that, because there is all this hidden back and forth. […] [researchers] expect to be able to hand over their protocol and then I will find them patients and those patients will be … representative and I will be able to talk to all of those patients and … write them up a report and …send it all back and they will be able to be like, “Thanks for the PPI”, and be on their merry way (P13).
What P13 communicates in this story is the researcher’s failure to perceive the difference between PPI work and institutional norms for project delivery: the researcher who asks for “some people with lived experience” is not simply underestimating how long this process will take. Rather, involvement work is perceived as homologous to metricized and institutionally recognizable activities (for example, recruitment to trials or producing project reports) for which there already exist standard procedures. Here, the relational complexity and improvised dynamic of involvement is turned into a deliverable (“the PPI”) that can be produced through following an appropriate procedure. When PPI workers are expected to instantly deliver the right contributors to fit the project needs, PPI labour is essentially black boxed and in its place sits “the PPI”, a kind of magical object seemingly conjured out of nowhere.
Such invisibility, however, may also be purposefully produced by the PPI workers themselves. One participant spoke of this at length, when detailing how they worked behind the scenes to ensure public contributors have input into research documents:
When we get a plain English summary from a researcher, we rewrite them completely. If the advisory group [see] … a really bad plain English summary, they are just going to go, “I don’t understand anything”. I might as well do the translation straight away so that they can actually review something they understand. [Researchers then] think, “Oh, [the public advisory group] are so good at writing” … and I am thinking, “Well, they don’t … write, they review, and they will say to me, ‘Maybe move this up there and that up there, and I don’t understand these’”, … They are great, don’t get me wrong, but they don’t write it. And it is the same with a lot of things. They think that [the group] are the ones that do it when it is actually the team (P7).
Here, the invisibility of the PPI worker’s labour is purposefully wrought to create good will and lubricate collaboration. Several participants said that they chose to engage in such purposeful invisibility because they knew that resources were not available to train researchers in plain writing and public contributors in academic writing. PPI workers, in ghost-writing accessible texts, thus effect a shortcut in the institutional labour required to generate alignment between researchers and public contributors. However, this shortcut comes at a price: in effecting it, PPI workers may collude in conjuring “the PPI” – they may themselves make their own work disappear.
“Not a 9 to 5”: PPI work as more than a job
Most participants reported that overtime working was common for themselves and their teammates, whether they were on a fractional or full-time contract. Overall, participants saw undertaking extra work as a necessary consequence of their commitment towards public contributors, a commitment which made it difficult to turn work down:
Everyone loses if you say no: the public contributors aren’t involved in a meaningful way, the project won’t be as good because it doesn’t have meaningful PPI involvement (P20).
While overwork was a common result of this commitment, some participants described such overwork as the feature that distinguished PPI work from what one commonly understands as a “job”, because, in this case, over-work was seen as freely chosen rather than externally imposed:
It is me pushing myself or wanting to get things done because I started it and I think I would get less done if I worked less and that would bother me, but I don’t think it is a pressure necessarily from [line manager] or [the institution] or anyone to be like, “No, do more” (P13).
Participants presented relationship building not only as the most time-consuming but also the most enjoyable aspect of PPI work. Community engagement was a key site for this and once again participants tended to represent this type of work as freely chosen:
I did most of the work in my free time in the end because you have to go into communities and you spend a lot longer there. […] So, all of that kind of thing I was just doing in my spare time and I didn’t really notice at the time because I really enjoyed it (P6).
Thus, time spent in relationship building was constituted as both work and not work. It did not lend itself to metricization via workplace time management and additionally, was not perceived by participants themselves as labour (“I didn’t really notice it at the time”). At the same time, out-of-hours work was rationalized as necessary for inclusivity, set up to enable collaboration with public contributors in so far as these do not have a contractual relationship to the employer:
That is not a 9–5. That is a weekends and holidays sort of job, because our job is to reduce the barriers to involvement and some of those barriers are hours – 9–5 is a barrier for some people (P17).
If working overtime allows PPI workers to reduce barriers and enable collaboration with those who are not employed by the institution, that same overtime work also serves to conceal the contractual nature of the PPI workers’ own labour, which now becomes absorbed into the moral requirements of PPI.
“Caught in the middle”: accountability without control
Participants repeatedly emphasized that their ability to contribute to research delivery was stymied by their lack of control over specific projects and over broader institutional priority setting:
… as a PPI lead we are not full member of staff, we are not responsible for choosing the research topics. We […] can only guide researchers who come to us and tell us what they are doing … we don’t have any power to define what the public involvement looks like in a research project (P6).
Tasked with creating alignments and partnerships between the publics and institutions, participants argued that they did not have the power to make them “stick” because they are not “really” part of the team. However, even as PPI workers lacked the power to cement partnerships, any failure in the partnership could be ascribed to them, perceived as a failure of the PPI worker by both funder and public contributors:
Often you have to hand over responsibility and the researcher [who] can let the panel down and … I feel like I have let the panel member down because … I am the one who said, “Oh yes, this person wants to talk to you”, and I find that really challenging, getting caught in the middle like that (P21).
This pairing of accountability with lack of control became more pronounced in grant applications or reports to the funder:
It is also quite frustrating in the sense that, just because I advise something, it doesn’t necessarily mean that it gets implemented or even included in the final grant. [even so] whatever the feedback is still reflects on us, not necessarily on the people who were making the wider decisions […] As PPI leads, we are still usually the ones that get the blame (P10).
Several participants testified to this double frustration: having to witness their PPI plans being rewritten to fit the constraints (financial, pragmatic) of the funding application, they then often found themselves held accountable if the PPI plans fail to carry favour with the funder. PPI workers then become the site where institutional accountability to both its public partners and to the funder gathers – it is as though, while located outside most decision-making, they nevertheless become the attractors for the institution’s missing accountability, which they experience, in the words of P21, as “ being caught in the middle ” or, as another participant put it, as “ the worry you carry around ” (P16).
“There to just get on with it”: delivering change without changing
Participants recognized that effective collaboration between research institutions and various publics requires fundamental institutional changes. Yet they also argued that while PPI workers are not themselves capable of effecting such change, there is nevertheless considerable institutional pressure to deliver on promises made in grant applications and build PPI strategies on this basis:
So, there is that tension about […] pushing this agenda and encouraging people to do more [….] rather than just accepting the status quo. But actually, the reality is that it is very, very hard to get everybody in [grant name] to change what they do and I can’t make that happen, [senior PPI staff] can’t make that happen, nobody can. The whole systemic issue … But you have got, somehow in the strategy and what you say you are going to do, that tension between aspiration and reality (P4).
This tension between aspiration and reality identified here could not be spelled out in reports for fear of reputational damage. In fact, the expectation to have delivered meaningful PPI, now routinely set up in NIHR applications, could itself militate against such change. For example, a frequently voiced concern was that PPI was being progressively under-resourced:
I feel the bar is getting higher and higher and higher and expectations are higher and we have got no extra resource (P16).
However, annual reports, the mechanism through which the doing of PPI is evidenced, made it difficult to be open about any such under-resourcing.
We will allude to [the lack of resources]. So, we will say things like, “We punch above our weight”, but I am not sure that message gets home to the NIHR very clearly. It is not like the annual report is used to say, “Hey, you’re underfunding this systematically, but here’s all the good stuff we do”, because the annual report is, by essence, a process of saying how great you are, isn’t it? (P3).
The inclusion of PPI as a “deliverable” meant that, in a competitive ecosystem, the pressure is on to report that PPI has always already been delivered. As another participant put it, “ no one is going to report the bad stuff ” (P17). Hence reporting, in setting up PPI as a deliverable, reinforced new zones of invisibility for PPI labour and made it harder to surface any under-resourcing for such labour. Furthermore, such reporting also played down any association between successful PPI and system transformation. Another participant described the resistance they encountered after arguing the organization should move away from “last-minute” PPI:
I think it is really hard when […] these people are essentially paying your pay cheque, to then try to push back on certain things that I don’t think are truly PPI ….[A]s somebody who I felt my role was really to show best practice, for then [to be] seen as this difficult person for raising issues or pushing back rather than just getting things done, is really hard [….] I get the impression, at least within the [organization] … that I am not there to really point out any of the issues. I am there just to get on with it (P14).
This opposition between pointing out the issues and “getting on with it” is telling. It names a contradiction at the heart of PPI labour: here, the very act of pushing back – in this case asking for a commitment to more meaningful and ongoing PPI – can be perceived as going against the PPI worker’s responsibilities, insofar as it delays and undoes team expectations for getting things done, for delivering PPI. Here, then, we find an exemplary instance of the incommensurability between the temporal demands of research and those of meaningful PPI practice.
How do the five themes we have presented help open out how policies around public participation are put into practice—as well as the contradictions that this practice navigates – in health systems organized by the rhetorical suturing of performance management onto public benefit? We have argued that the development of a dedicated workforce represents an attempt to “repair” the tension experienced by researchers between the administrative, facilitative and emotional work of PPI and the kinds of deliverables that the institution requires them to prioritize. We argue that our findings indicate that insofar as PPI workers’ role then becomes one of “delivering” PPI, this tension is reproduced and at times intensified within their work. This is because, as actors in the health research ecosystem, PPI staff are tethered to the very regimes of performance management, which give rise to an institutional misapprehension of the actual labour associated with delivering PPI.
This misapprehension surfaces in the instruments through which the funder costs, measures and generates accountability for PPI – namely, the requirement for a costed PPI lead and the mandatory inclusion of a PPI section in applications and regular reports to funder. The NIHR requirement for a costed PPI lead, intended to legitimize the undertaking of PPI as an integral part of a research team’s responsibilities, may instead continue to position the PPI worker as a site for the research team’s wholesale outsourcing of responsibility for PPI, since this responsibility, while in tension with other institutional priorities, cannot nevertheless be refused by the team. Furthermore, the use of titles such as lead, manager or co-ordinator not only signal an orderly distinction between junior and senior roles, which often does not apply in practice, but also reframes the extra-institutional work of PPI (the forging of relationships and administrative support with public contributors), through the intra-institutional functions of performance/project management. This reframing elides an important difference between the two: public and patient partners, for the most part, do not have a formal contractual relationship with the institution and are not subject to performance management in the way that contracted researchers and healthcare professionals are. Indeed, framing the relationship between PPI workers and public contributors through the language of “management” fundamentally misrecognizes the kinds of relationalities produced in the interactions between PPI workers and public contributors and elides the externality of PPI to the “logic of deliverables” [ 36 ].
The inclusion of a detailed PPI section in grant applications and annual reports to funder further consolidates this misapprehension by also representing public involvement as if it is already enrolled within organizational normative procedures and therefore compels those in receipt of funding to evidence such delivery through annual reports [ 37 ]. This demand puts PPI workers under increasing pressure, since their function is to essentially present PPI objectives as not only achievable but already achieved, thus essentially bracketing out the process of organizational transformation which is a necessary prerequisite to establishing enduring partnerships with patients and the public. This bracketing out is at work in the organizational expectation to “just get on with it”, which structures the labour of delivering PPI in NIHR-funded research. Here, the demand to just get on, to do the work one is paid to do, forecloses the possibility of engaging with the structural obstacles that militate against that work being done. To the extent that both role designation and reporting expectations function to conceal the disjuncture that the establishment of public partnerships represents for regimes of performance management, they generate new invisibilities for PPI workers. These invisibilities radically constrain how such labour can be adequately undertaken, recognized and resourced.
In suggesting that much of the labour of staff in public involvement roles is institutionally invisible, and that organizational structures may obstruct or block their efforts, we concur with the arguments made by Watermeyer, Mathie and colleagues about the position of staff in public engagement and public involvement roles, respectively. However, our account diverges from theirs in our interpretation of how and why this labour is experienced as invisible and how that invisibility could be remedied. Mathie and colleagues in particular attribute this invisibility to a lack of parity and an institutional devaluation of what are perceived as “soft skills” – facilitation and relationship building in particular [ 50 ]. They therefore seek to raise PPI work to visibility by emphasizing the complexity of PPI activities and by calling for a ring-fencing of resources and a development of infrastructures capable of sustaining such work. While we concur that the invisibility of PPI labour is connected to its devaluation within research institutions, we also suggest that, in addition, this invisibility is a symptom of a radical misalignment between regimes of performance management and the establishment of sustainable public partnerships. Establishing such partnerships requires, as a number of researchers have demonstrated [ 18 , 59 , 60 ], considerable institutional transformation, yet those tasked with delivering PPI are not only not in a position to effect such transformation, they are also compelled to conceal its absence.
Recognizing and addressing the misalignment between regimes of performance management and the establishment of sustainable public partnerships becomes particularly pressing given the increasing recognition, in many countries, that public participation in health research and intervention development is an important step to effectively identifying and addressing health inequalities [ 19 , 61 , 62 ]. Calls for widening participation, for the inclusion of under-served populations and for co-designing and co-producing health research, which have been gathering force in the last 20 years, have gained renewed urgency in the wake of the coronavirus disease 2019 (COVID-19) pandemic [ 63 , 64 , 65 , 66 , 67 ]. In the United Kingdom, Best Research for Best Health: The Next Chapter, published by the NIHR in 2021 to define the direction and priorities for NHS Research for the coming decade, exemplifies this urgency. The document asserts that a radical broadening of the scope of PPI (now renamed “public partnerships”) is essential for combatting health inequalities: it explicitly amplifies the ambitions of its 2006 predecessor by setting up as a key objective “close and equitable partnerships with communities and groups, including those who have previously not had a voice in research” [ 68 ]. Here, as in other comparable policy documents, emphasis on extending partnerships to so-called underserved communities rests on the assumption that, to some degree at least, PPI has already become the norm for undertaking research. This assumption, we argue, closes down in advance any engagement with the tensions we have been discussing in this paper, and in so doing risks exacerbating them. The document does recognize that for such inclusive partnerships to be established institutions must “work differently, taking research closer to people [..] and building relationships of trust over time” – though, we would suggest, it is far from clear how ready or able institutions are really to take on what working differently might mean.
Our study engages with and emphasizes this need to “work differently” while also arguing that the demands and expectations set up through regimes of performance management and their “logic of deliverables” are not favourable to an opening of a space in which “working differently” could be explored. In health research systems organized through these regimes, “working differently” is constrained by the application of the very templates, instruments and techniques which constitute and manage “business as usual”. Any ongoing effort to transform health research systems so as better to respond to growing health inequalities, our study implies, needs to combat, both materially and procedurally, the ease with which the disjuncture between embedding public partnerships and normative ways of undertaking research comes to disappear.
Limitations
We focus on the labour of the PPI workforce and their negotiation of performance management regimes, which means that we have not discussed relationships between PPI staff and public contributors nor presented examples of good practice. While these are important domains for study if we are to understand the labour of the PPI workforce, they lie outside the scope of this article. Furthermore, our focus on the UK health research system means that our conclusions may have limited generalizability. However, both the consolidation of NPM principles in public sector institutions and the turn to public and patient participation in the design and delivery of health research are shared developments across countries in the Global North in the last 40 years. Therefore, the tensions we discuss are likely to also manifest in health systems outside the United Kingdom, even as they may take somewhat different forms, given differences in how research and grants are costed, and roles structured. Finally, this project has elements of “insider” research since both authors, while working primarily as researchers, have also had experience of embedding PPI in research studies and programmes. Insider research has specific strengths, which include familiarity with the field and a sense of shared identity with participants which may enhance trust, facilitate disclosure and generate rich data. In common with other insider research endeavours, we have sought to reflexively navigate risks of bias and of interpretative blind spots resulting from over-familiarity with the domain under research [ 69 ] by discussing our findings and interpretations with “non-insider” colleagues while writing up this research.
Our qualitative study is one of the first to investigate how the UK PPI workforce is negotiating the current health research landscape. In doing so, we have focused on the UK’s NIHR since this institution embodied the redirection of performance management regimes towards public benefit by means of public participation. If PPI is set up as both the means of enabling this redirection and an outcome of its success, then the PPI workforce, the professional cadre evolving to support PPI, becomes, we argue, the site where the tensions of attempting this alignment are most keenly experienced.
We suggest that, while such alignment would demand a wholesale transformation of organizational norms, the regimes of performance management underpinning research ecologies may also work to foreclose such transformation, thus hollowing out the promise of patient-centred research policies and systems. Recognizing and attending to this foreclosure is urgent, especially given the current policy emphasis in many countries on broadening the scope, ambition and inclusivity of public participation as a means of increasing the reach, relevance and potential positive impact of health research.
Availability of data and materials
The data that support the findings of this study are available on request from the corresponding author.
Shippee ND, Domecq Garces JP, Prutsky Lopez GJ, Wang Z, Elraiyah TA, Nabhan M, et al. PMC5060820: patient and service user engagement in research: a systematic review and synthesized framework. Health Expect. 2015;18(5):1151–66.
Article PubMed Google Scholar
Domecq JP, Prutsky G, Elraiyah T, Wang Z, Nabhan M, Shippee N, et al. PMC3938901: patient engagement in research: a systematic review. BMC Health Serv Res. 2014;26(14):89.
Article Google Scholar
Crocker J, Hughes-Morley A, Petit-Zeman S, Rees S. Assessing the impact of patient and public involvement on recruitment and retention in clinical trials: a systematic review. In: 3rd International Clinical Trials Methodology Conference. 2015;16(S2):O91.
Staniszewska S, Herron-Marx S, Mockford C. Measuring the impact of patient and public involvement: the need for an evidence base. Int J Qual Health Care. 2008;20(6):373–4.
Brett J, Staniszewska S, Mockford C, Herron-Marx S, Hughes J, Tysall C, et al. Mapping the impact of patient and public involvement on health and social care research: a systematic review. Health Expect. 2014;17(5):637–50.
Staniszewska S, Adebajo A, Barber R, Beresford P, Brady LM, Brett J, et al. Developing the evidence base of patient and public involvement in health and social care research: the case for measuring impact. Int J Consum Stud. 2011;35(6):628–32.
Staley K. ‘Is it worth doing?’ Measuring the impact of patient and public involvement in research. Res Involv Engagem. 2015;1(1):6.
Article PubMed PubMed Central Google Scholar
Brady L, Preston J. How do we know what works? Evaluating data on the extent and impact of young people’s involvement in English health research. Res All. 2020;4(2):194–206.
Daly J. Evidence based medicine and the search for a science of clinical care. Oakland: University of California Press; 2005.
Book Google Scholar
Ward PR, Thompson J, Barber R, Armitage CJ, Boote JD, Cooper CL, et al. Critical perspectives on ‘consumer involvement’ in health research epistemological dissonance and the know-do gap. J Sociol. 2010;46(1):63–82.
Rose D, Kalathil J. Power, privilege and knowledge: the untenable promise of co-production in mental “health.” Front Soc. 2019;4(57):435866.
Google Scholar
Beresford P. PMC7317269: PPI or user Involvement: taking stock from a service user perspective in the twenty first century. Res Involv Engagem. 2020;6:36.
McKevitt C. Experience, knowledge and evidence: a comparison of research relations in health and anthropology. Evid Policy. 2013;9(1):113–30.
Boaz A, Biri D, McKevitt C. Rethinking the relationship between science and society: has there been a shift in attitudes to Patient and Public Involvement and Public Engagement in Science in the United Kingdom? Health Expect. 2016;19(3):592–601.
Green G. Power to the people: to what extent has public involvement in applied health research achieved this? Res Involv Engagem. 2016;2(1):28.
Miller FA, Patton SJ, Dobrow M, Berta W. Public involvement in health research systems: a governance framework. Health Res Policy Syst. 2018;16(1):79.
Madden M, Speed E. Beware zombies and unicorns: toward critical patient and public involvement in health research in a neoliberal context. Front Sociol. 2017;2(7):1–6.
Papoulias S, Callard F. Material and epistemic precarity: it’s time to talk about labour exploitation in mental health research. Soc Sci Med. 2022;306:115102.
Lignou S, Sheehan M, Singh I. ‘A commitment to equality, diversity and inclusion’: a conceptual framework for equality of opportunity in patient and public involvement in research. Res Ethics. 2024;20(2):288–303.
Dorey P. The legacy of Thatcherism—public sector reform. Obs Soc Br. 2015;17:33–60.
National Health Service and Community Care Act. 1990.
Ferlie E, Ashburner L, Fitzgerald L, Pettigrew A. The new public management in action. Oxford: Oxford University Press; 1996.
Lapuente V, Van de Walle S. The effects of new public management on the quality of public services. Governance. 2020;33(3):461–75.
Atkinson P, Sheard S, Walley T. ‘All the stars were aligned’? The origins of England’s National Institute for Health Research. Health Res Policy Syst. 2019;17(1):95.
Weir S, Beetham D. Political power and democratic control in Britain: the democratic audit of the United Kingdom. London: Psychology Press; 1999.
Sullivan HC, Skelcher C. Working across boundaries. 1st ed. Houndmills: Palgrave; 2002.
The new NHS: modern, dependable 1997.
Cutler T, Waine B. Managerialism reformed? New labour and public sector management. Soc Policy Adm. 2000;34(3):318–32.
Speed E. Applying soft bureaucracy to rhetorics of choice: UK NHS 1983–2007. In: Clegg SR, Harris M, Hopfl H, editors. Managing modernity: the end of bureaucracy? Oxford: Oxford University Press; 2011.
Dalingwater L. Post-new public management (NPM) and the reconfiguration of health services in England. Obs Soc Br. 2014;1(16):51–64.
Bennett C, McGivern G, Ferlie E, Dopson S, Fitzgerald L. Making wicked problems governable? The case of managed networks in health care. 1st ed. Oxford: Oxford University Press; 2013.
Hanney S, Kuruvilla S, Soper B, Mays N. Who needs what from a national health research system: lessons from reforms to the English department of Health’s R&D system. Health Res Policy Syst. 2010;13(8):11–11.
Evans TW. Best research for best health: a new national health research strategy. Clin Med. 2006;6(5):435–7.
DeNegri S, Evans D, Palm M, Staniszewka S. The history of INVOLVE—a witness seminar. 2024. https://intppinetwork.wixsite.com/ippin/post/history-of-involve . Accessed Apr 17 2024.
Evans D, Pollard KC. Theorising service user involvement from a researcher perspective. In: Staddon P, editor. Mental health service users in research United States. Bristol: Policy Press; 2013. p. 39.
Papoulias SC, Callard F. ‘A limpet on a ship’: spatio-temporal dynamics of patient and public involvement in research. Health Expect. 2021;24(3):810–8.
Komporozos-Athanasiou A, Paylor J, McKevitt C. Governing researchers through public involvement. J Soc Policy. 2022;51(2):268–83.
Paylor J, McKevitt C. The possibilities and limits of “co-producing” research. Front Sociol. 2019;4:23.
Boylan AM, Locock L, Thomson R, Staniszewska S. “About sixty per cent I want to do it”: health researchers’ attitudes to, and experiences of, patient and public involvement (PPI)—a qualitative interview study. Health Expect. 2019. https://doi.org/10.1111/hex.12883 .
DeNegri S. Going the extra mile: improving the nation’s health and wellbeing through public involvement in research. 2015.
Crowe S, Wray P, Lodemore M. NIHR public involvement leads’ meeting November 25 2016. 2017.
NIHR. Taking stock—NIHR public involvement and engagement. 2019. https://www.nihr.ac.uk/documents/taking-stock-nihr-public-involvement-and-engagement/20566 . Accessed Apr 28 2023.
NIHR. Definition and role of the designated PPI (Patient and Public Involvement) lead in a research team. 2020. https://www.nihr.ac.uk/documents/definition-and-role-of-the-designated-ppi-patient-and-public-involvement-lead-in-a-research-team/23441 . Accessed Apr 28 2023.
Li KK, Abelson J, Giacomini M, Contandriopoulos D. Conceptualizing the use of public involvement in health policy decision-making. Soc Sci Med. 2015;138:14–21.
Staley K, Barron D. Learning as an outcome of involvement in research: what are the implications for practice, reporting and evaluation? Res Involv Engagem. 2019;5(1):14.
Brady L, Miller J, McFarlane-Rose E, Noor J, Noor R, Dahlmann-Noor A. “We know that our voices are valued, and that people are actually going to listen”: co-producing an evaluation of a young people’s research advisory group. Res Involv Engagem. 2023;9(1):1–15.
Knowles S, Sharma V, Fortune S, Wadman R, Churchill R, Hetrick S. Adapting a codesign process with young people to prioritize outcomes for a systematic review of interventions to prevent self-harm and suicide. Health Expect. 2022;25(4):1393–404.
Mathie E, Wythe H, Munday D, Millac P, Rhodes G, Roberts N, et al. Reciprocal relationships and the importance of feedback in patient and public involvement: a mixed methods study. Health Expect. 2018;21(5):899–908.
Wilson P, Mathie E, Keenan J, McNeilly E, Goodman C, Howe A, et al. ReseArch with Patient and Public invOlvement: a RealisT evaluation—the RAPPORT study. Health Serv Deliv Res. 2015;3(38):1–176.
Article CAS Google Scholar
Mathie E, Smeeton N, Munday D, Rhodes G, Wythe H, Jones J. The role of patient and public involvement leads in facilitating feedback: “invisible work.” Res Involv Engagem. 2020;6(1):40.
Watermeyer R, Rowe G. Public engagement professionals in a prestige economy: ghosts in the machine. Stud High Educ. 2022;47(7):1297–310.
Watermeyer R, Lewis J. Institutionalizing public engagement through research in UK universities: perceptions, predictions and paradoxes concerning the state of the art. Stud High Educ. 2018;43(9):1612–24.
Collinson JA. ‘Get yourself some nice, neat, matching box files!’ research administrators and occupational identity work. Stud High Educ. 2007;32(3):295–309.
Braun V, Clarke V. Reflecting on reflexive thematic analysis. Qual Res Sport Exerc Health. 2019;11(4):589–97.
Clarke V, Braun V. Thematic analysis: a practical guide. 2021.
Clarke V, Braun V. Successful qualitative research. London: SAGE; 2013.
Lincoln YS, Guba EG. Naturalistic inquiry. 3rd ed. Beverly Hills: Sage Publications; 1985.
Kaiser K. Protecting respondent confidentiality in qualitative research. Qual Health Res. 2009;19(11):1632–41.
Heney V, Poleykett B. The impossibility of engaged research: complicity and accountability between researchers, ‘publics’ and institutions. Sociol Health Illn. 2022;44(S1):179–94.
MacKinnon KR, Guta A, Voronka J, Pilling M, Williams CC, Strike C, et al. The political economy of peer research: mapping the possibilities and precarities of paying people for lived experience. Br J Soc Work. 2021;51(3):888–906.
Bibbins-Domingo K, Helman A, Dzau VJ. The imperative for diversity and inclusion in clinical trials and health research participation. JAMA. 2022;327(23):2283–4.
Washington V, Franklin JB, Huang ES, Mega JL, Abernethy AP. Diversity, equity, and inclusion in clinical research: a path toward precision health for everyone. Clin Pharmacol Ther. 2023;113(3):575–84.
Graham ID, McCutcheon C, Kothari A. Exploring the frontiers of research co-production: the Integrated Knowledge Translation Research Network concept papers. Health Res Policy Syst. 2019;17(1):88.
Marten R, El-Jardali F, Hafeez A, Hanefeld J, Leung GM, Ghaffar A. Co-producing the covid-19 response in Germany, Hong Kong, Lebanon, and Pakistan. BMJ. 2021;372: n243.
Smith H, Budworth L, Grindey C, Hague I, Hamer N, Kislov R, et al. Co-production practice and future research priorities in United Kingdom-funded applied health research: a scoping review. Health Res Policy Syst. 2022;20(1):36.
World Health Organization. Health inequity and the effects of COVID-19: assessing, responding to and mitigating the socioeconomic impact on health to build a better future. Copenhagen: Regional Office for Europe. World Health Organization; 2020.
Dunston R, Lee A, Boud D, Brodie P, Chiarella M. Co-production and health system reform—from re-imagining to re-making. Aust J Public Adm. 2009;68:39–52.
Department for Health and Social Care. Best research for best health: the next chapter. Bethesda: National Institute for Health Research; 2021.
Wilkinson S, Kitzinger C. Representing our own experience: issues in “insider” research. Psychol Women Q. 2013;37:251–5.
Download references
Acknowledgements
S.P. presented earlier versions of this paper at the 8th annual conference of the Centre for Public Engagement Kingston University, December 2021; at the Medical Sociology conference of the British Sociological Association, September 2022; and at the annual Health Services Research UK Conference, July 2023. They are grateful to the audiences of these presentations for their helpful comments. Both authors are also grateful to the generous participants and to the NIHR Applied Research Collaboration Public Involvement Community for their sustaining support and encouragement during this time. S.P. also wishes to thank Felicity Callard for her comments, advice and suggestions throughout this process: this paper would not have been completed without her.
S.P. is supported by the National Institute for Health and Care Research (NIHR) Applied Research Collaboration (ARC) South London at King’s College Hospital NHS Foundation Trust. The views expressed are those of the author and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
Author information
Authors and affiliations.
Health Service & Population Research, King’s College London, London, United Kingdom
Stan Papoulias
Centre for Public Health and Community Care, University of Hertfordshire, Hatfield, United Kingdom
Louca-Mai Brady
You can also search for this author in PubMed Google Scholar
Contributions
S.P. developed the original idea for this article through earlier collaborations with L.M.B. whose long-term experience as a PPI practitioner has been central to both the project and the article. L.M.B. contributed to conceptualization, wrote the first draft of the background and undertook revisions after the first draft including reconceptualization of results. S.P. contributed to conceptualization, undertook data analysis, wrote the first draft of findings and discussion and revised the first draft in its entirety in consultation with L.M.B. Both authors read and approved the final manuscript.
Corresponding author
Correspondence to Stan Papoulias .
Ethics declarations
Ethics approval and consent to participate.
The study received a favourable opinion from the Psychiatry, Nursing and Midwifery Research Ethics Panel, King’s College London (ref no.: LRS-20/21-21466).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Papoulias, S., Brady, LM. “I am there just to get on with it”: a qualitative study on the labour of the patient and public involvement workforce. Health Res Policy Sys 22 , 118 (2024). https://doi.org/10.1186/s12961-024-01197-5
Download citation
Received : 17 July 2023
Accepted : 26 July 2024
Published : 02 September 2024
DOI : https://doi.org/10.1186/s12961-024-01197-5
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Patient and public involvement
- PPI workforce
- New public management
- National Institute for Health and Care Research (NIHR)
Health Research Policy and Systems
ISSN: 1478-4505
- Submission enquiries: Access here and click Contact Us
- General enquiries: [email protected]
- Advanced search

Advanced Search
Unpacking complexity in addressing the contribution of trauma to women’s ill health: a qualitative study of perspectives from general practice
- Find this author on Google Scholar
- Find this author on PubMed
- Search for this author on this site
- ORCID record for Jennifer MacLellan
- ORCID record for Sharon Dixon
- ORCID record for Francine Toye
- ORCID record for Abigail McNiven
- Figures & Data
Background There is an intricate relationship between the mind and the body in experiences of health and wellbeing. This can result in complexity of both symptom presentation and experience. Although the contribution of life trauma to illness experience is well described, this is not always fully recognised or addressed in healthcare encounters. Negotiating effective and acceptable trauma-informed conversations can be difficult for clinicians and patients.
Aim To explore the experience of primary care practitioners caring for women through a trauma-informed care lens.
Design and setting Qualitative study in the general practice setting of England, with reflections from representatives of a group with lived experience of trauma.
Method This was a secondary thematic analysis of 46 qualitative interviews conducted online/by telephone to explore primary care practitioners’ experiences of supporting women’s health needs in general practice, alongside consultation with representatives of a lived-experience group to contextualise the findings.
Results Four themes were constructed: ‘you prioritise physical symptoms because you don’t want to miss something’; you do not want to alienate people by saying the wrong thing; the system needs to support trauma-informed care; and delivering trauma-informed care takes work that can have an impact on practitioners.
Conclusion Primary care practitioners are aware of the difficulties in discussing the interface between trauma and illness with patients, and request support and guidance in how to negotiate this supportively. Lack of support for practitioners moves the focus of trauma-informed care from a whole-systems approach towards individual clinician–patient interactions.
- biopsychosocial models
- communication
- general practice
- trauma-informed care
- Introduction
As evident in the Women’s Health Strategy for England 1 and its underlying public consultation, 2 women’s health is complex and embedded in historical dismissal and stigma. There is an intricate relationship between the mind and the body in experiences of health and wellbeing. One facet of this complexity includes the possible contribution of trauma to the woman’s illness experience. The physical response to, and pathways of bodily damage as a result of, the hormonal environment of chronic stress has revealed links between unresolved emotional distress and autoimmune conditions. 3 Trauma has an impact on people in different ways. Although some people make positive adjustments, others experience mental ill health and/or develop physical symptoms from emotional distress. 4 This can result in complexity both in symptom presentation and health experience.
Trauma can result from an event, series of events, or set of circumstances that is experienced by an individual as harmful or life threatening and can include past experiences of care (including in maternity), adverse childhood events (ACEs), and other life experiences as an adult. ACEs are stressful or traumatic events that occur specifically during childhood or adolescence 5 and can include: abuse (physical, emotional, and sexual); neglect; living in a household with domestic violence, experience of illness, or bereavement. 6 In a systematic review and meta-analysis of 96 studies of adult health behaviours, the risk of poorer health outcomes (including cardiovascular disease, respiratory disorders, gastrointestinal disorders, and mental ill health) increased with the number of ACEs. 4 Experiences of trauma at any stage in life can cause lasting adverse effects on health. 3 In the UK, women are disproportionally affected by violence (twice as likely as men to experience domestic violence), 7 , 8 trauma, 9 , 10 and ill health, 11 , 12 highlighting the potential complexity of women’s health presentation.
Although the contribution of life trauma to illness experience is well described, primary care professionals do not always fully address it. Potential reasons include clinician concerns about missing a serious illness in a complex presentation or about alienating or upsetting the patient. 11 Addressing trauma often necessitates introducing conversations about the link between mind and body, which can be difficult to navigate. Significant challenges and uncertainties reside in how best to manage the link between mind and body in communication with patients and in healthcare pathways. Qualitative research indicates that primary care professionals can find it challenging to navigate this mind–body presentation. Suggestions from primary care professionals that physical symptoms are amplified by (or a manifestation of) distress can be experienced as dismissal and invalidation by patients. 13 – 15 Attempts to bridge these health needs are therefore not always experienced as supportive. This illustrates the potential challenges of negotiating trauma-informed conversations in ways that are experienced as acceptable and supportive by patients.
| Significant challenges and uncertainties reside in how best to manage the link between mind and body in communication with patients and in healthcare pathways. Lack of supportive resources to deliver holistic, trauma-informed care risks practitioners (inadvertently) avoiding discussion of the contribution of distress in the illness presentation. A trauma-informed systems-level approach would support integration of psychological support within multiple care pathways and support wellbeing of practitioners providing care. |
How this fits in
Trauma-informed care is a framework founded on five core practices: safety, trustworthiness, choice, collaboration, and empowerment. These can be used to address the impact of trauma on patients and healthcare professionals and prevent re-traumatisation in healthcare services. 16 However, definitions, guidance, practitioner training, delivery, and support for trauma-informed approaches vary between healthcare settings according to local-level funding priorities with implementation described as disjointed. 16 Little is known about how healthcare professionals experience trying to effectively deliver trauma-informed care. The aim of this study was to explore the experiences of primary care practitioners caring for women through a trauma-informed care lens.
This study was a secondary analysis of qualitative interview data gathered to explore primary care practitioners’ experiences of supporting women’s health needs in primary care. Between March and September 2022, we interviewed a sample of 46 primary care practitioners across England (GPs n = 31, nurses n = 9, other professionals n = 6, with an average of 12 years’ experience [1 to 30 years], 41/46 female), ensuring representation from practices working in areas of deprivation where health inequalities and multimorbidity are significant challenges. Detailed methods and participant characteristics of the parent study are reported elsewhere. 17
The original topic guide was developed by three authors in response to a perceived gap in knowledge about women’s health care in primary care and commissioned by the National Institute of Health Research (NIHR) Policy Research Programme. Data were collected through single-episode, one-to-one interviews with fully informed consent. They were conducted virtually online or by telephone by two experienced qualitative researchers and audio-recorded. These were transcribed verbatim, checked against the original recording, and thematically analysed.
The team then undertook a focused enquiry using secondary thematic analysis of the dataset to explore primary care professionals’ navigation of women’s experiences of distress as a contribution to their symptoms. 18 We recoded the transcripts line-by-line where distress, emotional, or psychological impact or contribution to health experience was mentioned. We discussed the constructed data categories within the research team to create interpretive themes. We reflected on these themes with representatives of three charities supporting women with significant experience of historical and contemporary trauma to add a lived-experience perspective to the data.
Four themes were constructed from the data:
‘you prioritise physical symptoms because you don’t want to miss something’;
you do not want to alienate people by saying the wrong thing;
the system needs to support trauma-informed care; and
delivering trauma-informed care takes work that can have an impact on practitioners.
Theme 1: ‘you prioritise physical symptoms because you don’t want to miss something’ (PC30, female [F], GP for 5 years)
Practitioners described women’s health consultations as often complex and difficult to manage in a single, constrained time slot. A significant concern was the fear of missing a physical condition requiring specific or prompt treatment as many women’s health complaints could present with similar but vague symptomatology and could suggest multiple possible diagnoses. Some participants reflected that a challenge of navigating diagnostic processes, by first excluding potential causes that need specific interventions such as cancer, meant the contribution of distress to physical symptoms was pushed down the list of considerations: ‘It’s definitely sort of a symptom sieve to start with, and to adequately hear your patient and really hear them and really listen to what they’re saying […] There are many things that are difficult to do in ten minutes, but I … women’s health is particularly difficult.’ (PC17, F, advanced nurse practitioner [ANP] for more than 15 years) ‘They’re often quite vague symptoms: bloating, things like that, so you either have a very low index of suspicion and you’re seeing ca-125s [blood test that may indicate ovarian cancer] and you’re scanning everybody, or things get missed, and [sighs] yeah, it can be very challenging and obviously if you miss something like that it’s devastating for everybody involved, but it’s very difficult.’ (PC12, F, GP for more than 15 years)
Participants described how investigation pathways move through a hierarchy of potential causes and may involve a stepped process that did not always yield a confirmatory or unifying diagnosis. This meant that the participants had to manage patients’ expectations of diagnosis throughout this process.
Theme 2: you do not want to alienate people by saying the wrong thing
Some felt that a cultural shift was needed for the wider healthcare system to acknowledge the mind–body interplay as a legitimate expression of distress, to support practitioners to discuss this with their patients along their care pathway, and to provide timely access to psychological support services: ‘Perhaps some of training for staff would be about how you talk about the connection between your brain and your body […] without sounding dismissive and actually, training individuals to become more sensitive to these types of, conversations.’ (PC46, male [M], GP for 15 years)
However, some felt that patients were not always receptive to recognising the contribution of emotions or past experiences to physical symptoms, the idea of an integral link between mind and body, or the offer of psychological support to cope with the distress of physical symptoms. Some participants were worried about alienating women who might interpret this suggestion as devaluing or de-legitimising their symptom experience, and were therefore sometimes unsure when or how to navigate this: ‘I don’t think many patients like it when we end up going down that route when it comes to pain, any pain, not just pelvic pain in itself, because they want a diagnosis of some form or another, whatever it’s called, rather than being given some antidepressants or some counselling.’ (PC18, F, GP for 10 years)
Participants described the essential first step to be validation of the woman’s experience, emphasising understanding and genuine belief in the symptoms as ‘real’ (although perhaps currently unexplained) before exploring the impact of trauma or life stress in its aetiology: ‘It’s just spending the time with them and actually acknowledging, yes the pain is real, but are we not just saying you know, “you’ve got pain and we can’t find any cause for it”, “the pain is actually real”, and what we can do is maybe go down the route of psychological sort of therapy for that, that might be the best route of managing it.’ (PC18, F, GP for 10 years) ‘The first lady I was talking about absolutely wasn’t having any of it […] I got her some interesting resources […] and I just mis-pitched it […] the fact that this is her body feeling overwhelmed and feeling overwhelmed with the difficulties in her life and how to explain that in a way that seems scientific … it’s quite difficult, isn’t it?’ (PC14, F, GP for 1 year)
Healthcare professionals were aware and worried that exploring the contribution of trauma or distress in the physical symptom experience and that physical and emotional symptoms can coexist was not always well received. Restricted time in consultations highlighted the need for resources that could support this mind–body understanding in a positive and affirming way for the patient: ‘Often there is something organic, or something organic that has started it off, but then it often becomes this kind of complex combination of physical and then also psychological symptoms together, and I think kind of having resources to explain how psychological symptoms can impact pelvic pain […] I think kind of having good resources to try and back up what I’m saying would be quite helpful.’ (PC21, F, GP for more than 20 years)
Participants described how the net effect of these considerations could result in practitioners (inadvertently) avoiding discussion of the contribution of distress in the illness presentation: ‘ […] I think you can shut it down easily and not get emotionally involved, but you do not actually solve any of the issues unless they are straight up, simple, physical problems that you can just treat, but for the most part it doesn’t work very well.’ (PC30, F, GP for 5 years)
Participants recognised the importance of a trauma-informed approach in the complex and holistic care needs of women’s health. This extended to considerations about trauma-informed approaches to physical examination and how this could be enabled. Some highlighted the unique position of the primary care practitioner, in a potentially protracted diagnostic or support pathway, to communicate the contribution of distress in a supportive and helpful way to their patients.
Theme 3: the system needs to support trauma-informed care
Participants described four systemic challenges to the provision of trauma-informed care:
inadequate time allocated for appointments;
waiting times for specialist practitioner review in secondary care;
limited access to services; and
providing care for women returning from secondary care without a unifying diagnosis.
The challenges of time were frequently reported by participants: ‘I already know that I can’t do everything for you [the patient] in ten minutes, which isn’t always like a nice feeling for me, because we want to be able to help and you know do that within the time … who knows when they’ll be able to get an appointment again or you don’t want it to be frustrating for them, but equally you don’t want to rush yourself.’ (PC35, F, GP for less than 6 months) ‘They come back two months later and say, “I’ve still … I’m still … still haven’t seen the hospital”, and that there’s a certain amount of workload in primary care just because of … just because secondary care can’t take that on.’ (PC23, M, GP for more than 20 years)
In some areas they reported limited access to services such as counselling or psychological support services and community gynaecology because of local funding models and the challenges of providing care for women returning from secondary care without a unifying diagnosis. This often led to practitioners ‘holding the distress’ of the woman (see theme 4). Despite the challenges identified, participants described how they worked within the system constraints to offer the best service for their patients, for example, planning activities across multiple appointments: ‘In fifteen minutes it’s quite challenging, or if I’m trying to examine somebody […] that’s difficult, that’s when I sometimes ask them […] to come back for the examination so that I can do all the other things that are needed.’ (PC25, F, GP for 25 years)
Participants spoke of the structural supports that were in place that worked well in their efforts to deliver trauma-informed care, such as support networks, the ‘advice and guidance’ contact service to access secondary care (a system where GPs can access specialist advice before or instead of referral), and working with social prescribers (link workers who help patients to access non-medical support services in their community): ‘I mean advice and guidance [are] probably helpful I think, you write and you say, “What do I do?” and they tell you, and you then say to the patient, “this is what the specialist has said”, and that’s great, and that’s a really good idea.’ (PC23, M, GP for more than 20 years) ‘[Access to a social prescriber] is definitely making a difference; I don’t know what we did before to be quite honest. I don’t know what we would do because it’s just improved the quality of life for our patients, and it’s just helped us cope because you know we often see mental health problems, social problems, and with such a limited time constraint, limited resources, now that investment has been put in, it is definitely making a difference.’ (PC16, F, ANP for more than 18 years)
Theme 4: delivering trauma-informed care takes work and can have an impact on practitioners
Taking a trauma-informed approach relied heavily on the practitioner–patient relationship and some felt that the impact on practitioners was not always accounted for. The work involved in taking a trauma-informed approach to care had an impact on clinician workload. When they were able to navigate this challenge participants reported job satisfaction that was a positive impact. Conversely, when participants were unable to deliver the care they aspired to and believed they should, this had a negative impact. Protracted routes to diagnosis (or not getting a diagnosis), exacerbated by long waits to access specialist review in secondary care, left participants ‘holding the distress’ of women managing symptoms while they waited for a management plan: ‘I mean typically what happens is when a referral is done, the patient is waiting three, four, five months to be seen sometimes, but the patient’s still got those symptoms, so what do they do?’ (PC18, F, GP for 10 years) ‘So pain is complex. I think every pain service in the country is poorly funded and poorly accessible […] The challenge we have is these patients are constantly accessing us and, you know, I don’t want to label anything but they do end up becoming frequent attenders, which you know … and all we are is becoming a holding person in all of this.’ (PC46, M, GP for 15 years)
This increased the pressure on primary care practitioners who were operating without adequate system support. Although participants knew that managing uncertainty was integral to the role of the primary care practitioner, holding distress added to the challenge of appropriately broaching or exploring the mind–body link. Participants described feeling overwhelmed and personally affected by managing the expectations of patients held in limbo and holding their distress: ‘Women who have complex, like intractable symptoms that have been investigated and no one’s really come up with anything […] it’s more psycho-social input that’s needed, and they’ve seen a gynaecologist and they’re still struggling and there’s not really a solution, and so they’re … they’re the ones who you think, “oh my gosh, I … I’m … I’m not sure what I can offer … offer you”.’ (PC34, F, GP for 15 years) ‘I mean women’s health is a prime one, it causes so much anxiety, stress, impact on the family, and I think with the complexities around the referral pathways and who’s doing what, which has been one of my biggest stresses, people can fall through the gaps very easily.’ (PC26, F, GP for 5 years)
Participants sought support from colleagues within their daily work routines to reflect on clinical questions or patients with complex cases. However, some felt that there were limited support services for practitioners’ mental wellbeing in a more formalised and structured way: ‘We have our annual appraisal but that is very much to make sure that we’re not total lunatics […] but other than that […] they do support us, but they … you know it’s once a year, there’s no capacity to debrief on individual challenging cases or anything like that, it’s very much to check-in that we are sort of on the rails.’ (PC30, F, GP for 5 years)
Participants described how not being able to deliver high-quality, holistic care because of structural constraints was unsatisfying and challenging: ‘I was so unhappy in my previous job really, I’d say we still had support, but the patients were a lot more demanding and it just comes with that, you know a lot more child protection issues safeguarding and it … you know, it’s just a really challenging job and that, and not necessary work satisfying either.’ (PC04, F, GP for 3 years)
Lack of personal and systems support for practitioners moves the focus of trauma-informed care from a whole-systems approach to the clinician–patient interaction.
Our findings indicate that clinicians are aware of the contribution of trauma and distress to the presentation of physical symptomatology within women’s health consultations but that conversations about this could be difficult. Some participants felt confident and willing to discuss the role of distress in symptom presentation; others felt that these conversations were difficult and sometimes avoided the topic. Constraints such as limited time in consultations and the training and resources to facilitate discussions about the minded-body (the interconnection of physical and emotional health) and the role of trauma and distress could mean that clinicians did not always talk to patients about the impact of distress. This was exacerbated by system constraints such as limited support services for referral. Practitioners described building support mechanisms for themselves at work through debrief and clinical conversations with colleagues but told us that there were no formal supervision or support services routinely available for practitioners. The heavy work and emotional labour within an unsupportive system was described as contributing to practitioner frustration and burnout. Although patient relationships were framed within a trauma-informed lens, the organisational configuration was not always supportive to a trauma-informed approach.
Strengths and limitations
The use of secondary analysis has allowed us to conduct a focused analysis on a rich dataset of primary care professionals’ interviews. As this was done within the project timeline by the original research team, potential ethical concerns about the impact of the sociopolitical context that often accompanies secondary analysis were mitigated. 18 We were able to minimise participant burden and engage with a targeted group of women for whom trauma-informed care and its delivery has an immediate impact.
The principal limitation of our study is the restrictions offered by the original interview scope and guiding questions of the parent study that focused on women’s health. We are unable to report on experience in other areas of health care or by gender of care provider as this is unexplored. Gender was recorded; there were four male and 42 female responders. We purposively selected practitioners with an interest in women’s health rather than sampling an equally gender-split sample to derive patterns of experience that could be attributed to gender issues.
Comparison with existing literature
The link between trauma and ill health is well discussed in the literature, as are the principles of trauma-informed care. However, there appears to be little evidence of the clinician’s experience in discussing the interface between trauma and complexity with patients. The complexity of women’s health experiences challenges a dualistic approach to care and could respond better to the continuity model of primary care. 19 Practitioners in our data actively enacted the principles of trauma-informed care (such as safety, trustworthiness, and collaboration) in their personal practice with women. 16 However, the structural configuration of primary care services could complicate these care aspirations including when resources were limited or services were not flexible enough to support practitioner autonomy, which could hinder opportunities for timely care or follow-up. This could erode the practitioner’s efforts to deliver trauma-informed care, with potential consequences for both patients and clinicians. Such structural constraints in a climate of overwork are powerful sources of moral distress and burnout in studies of nurses, midwives, and doctors. 20 – 23 The risk of exposing practitioners to such moral distress can lead to the experience of vicarious trauma and reduced job satisfaction as they navigate the challenge of exploring the minded-body link with patients on their illness journey. 24 , 25 Primary care practitioners held women’s distress while they waited for specific therapies or supports, and yet the practitioners did not have adequate formal support systems to take care of their own wellbeing. This finding resonates with Pereira Gray et al , 25 who suggest that the UK shortage of GPs, erosion of continuity of care, sustained increase of remote consultation methods, and lack of structural support in the system may exacerbate challenges faced by practitioners to provide high-quality care. 26 – 28
Implications for research and practice
Our findings suggest that moving towards a trauma-informed systems-level approach would support integration of psychological support within multiple care pathways. A coordinated systems approach should support an integrated and holistic approach rather than encouraging a dichotomising split between physical or psychological services. Our findings suggest that this model would also support the wellbeing of practitioners delivering care and may have an impact on staff retention, making this a critical consideration at all system and service levels from individuals to practices to funders and commissioners. 28 , 29 However, less is known about how to enact or enable trauma-informed care at a systems level. 16 More research is needed about how to implement and support equitable, proportionate trauma-informed care in practice. This includes learning how to actively nurture equitable care within services, practices, and within primary care networks. At a funding and commissioning level, autonomy and equitable work need to be valued and enabled, and this requires policy attention; simplistic metrics of care such as numbers seen or a narrow focus on numerically quantifiable access will not capture either the impact on patients or practitioners. 28 Nor will this capture the contacts and appointments that did not happen. Furthermore, critical to effective equitable care is that practitioners need meaningful access to services that they can refer into and that will respond promptly and supportively to the needs identified. Work in areas of care such as female genital mutilation and domestic violence and abuse demonstrate that having acceptable accessible services to refer into enabled inquiry and compassionate care. 30 , 31 It is an ethical prerogative that trauma-informed enquiry is supported by trauma-informed services and support. Finally, support for staff is essential and the responsibility for this should not be devolved to individuals but commissioned and provided for. This contrasts with current policy, such as the wellbeing Quality and Outcomes Framework indicators that arguably devolve the responsibility for wellbeing to those in need of wellbeing support, without offering any tangible resources.
Healthcare professionals are aware of the difficulties in discussing the interface between trauma and complexity with patients 32 and our work shows they are requesting support and guidance in how to negotiate this supportively. The British Medical Association moral injury report 22 recommends systems changes that map onto the principles of trauma-informed care, including increased staffing, streamlining of bureaucracy, open and sharing work cultures, and provision of support for employees. However, although these recommendations acknowledge the problem and offer solutions, there is no requirement for organisations to address these structural concerns. Lack of these system supports for practitioners moves the focus of trauma-informed care from a whole-systems approach to the clinician–patient interaction. 16
To seek lived-experience perspectives on our findings, 33 we spoke with three representatives of charities supporting survival sex workers (SSW) in different regions of England as an exemplar vulnerable group with significant experience of historical and ongoing trauma. They told us how women experience stigma and are afraid of disclosure and confidentiality, particularly if their children have been removed and placed into social care. The charity representatives described how women engaged in SSW rarely sought medical care or achieved registration at a general practice surgery because of lifestyle circumstances and stigmatising experiences.
We asked what trauma-informed care looked like for their service and asked them to reflect on our findings. They recommended a systems-level approach to the delivery of trauma-informed services across the health service. Barriers to access were described as starting at the front door of the general practice surgery with the reaction of the receptionist. A lack of confidentiality in the reception area, closed consulting room doors, short consultation times, and the predominance of digital access methods for appointments were also cited. Beyond these, they suggested responsive, transparent pathways into support services for vulnerable women or those living in extreme circumstances would illustrate a trauma-informed approach to services. Individual practitioners were credited with adopting a trustworthy, trauma-informed approach but charity representatives, in consultation with the women they support, felt that the healthcare system could counteract individual good practice.
- Acknowledgments
We would like to acknowledge the contributions of our Public Involvement participants and express our thanks for the insights they shared with the research team.
This study was funded by the National Institute for Health and Care Research (NIHR) Policy Research Programme (NIHR202450). The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Ethical approval
This study has received ethical approval from the Health Research Authority (ref 22/HRA/0985).
The authors do not have ethical permission to share their dataset beyond the study team.
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article:
bjgp.org/letters
- Received January 12, 2024.
- Revision requested February 19, 2024.
- Accepted April 9, 2024.
- © The Authors
This article is Open Access: CC BY 4.0 licence ( http://creativecommons.org/licences/by/4.0/ ).
- Department of Health and Social Care
- Fairweather D ,
- Pearson WS ,
- Petruccelli K ,
- Di Lemma L ,
- Davies AR ,
- Dohrenwend BP
- Office for National Statistics (ONS)
- Andrews AR ,
- Jobe-Shields L ,
- Eckstrand KL ,
- Alessi EJ ,
- NHS England
- Chew-Graham CA ,
- Heyland S ,
- Kingstone T ,
- MacLellan J ,
- Ruggiano N ,
- Machtinger EL ,
- Shohaimi S ,
- Khaledi-Paveh B ,
- McKeller L ,
- Fleet J-A ,
- British Medical Association
- Molinaro ML ,
- Agarwal G ,
- Kokokyi S ,
- Pereira Gray D ,
- Sidaway-Lee K ,
- De Simona A ,
- Szilassy E ,
- Vennik JL ,
- NIHR School for Primary Care Research
In this issue

- Table of Contents
- Index by author
Thank you for recommending British Journal of General Practice.
NOTE: We only request your email address so that the person to whom you are recommending the page knows that you wanted them to see it, and that it is not junk mail. We do not capture any email address.
Citation Manager Formats
- EndNote (tagged)
- EndNote 8 (xml)
- RefWorks Tagged
- Ref Manager

- Tweet Widget
- Facebook Like
- Google Plus One
Jump to section
More in this toc section.
- Trends in clinical workload in UK primary care 2005–2019: a retrospective cohort study
- Information needs for GPs on type 2 diabetes in Western countries: a systematic review
- Support for primary care prescribing for adult ADHD in England: national survey
Related Articles
Cited by....

British Journal of General Practice
Choosing the correct interview type
The Live Interviews in UXtweak include two main interview types: Study Interview and Freeform Interview . Here you can learn when you should use which interview type.
Study Interview
This interview type is directly bound to a specific UX research approach. You should choose this type of interview when your study is focused on one research approach and you want to have the same structure of the interview for all participants. The Study Interviews are all about the study which is connected to the interview.
When you create a study interview, you need to choose one of the 9 available study types .
The setup of your chosen study type is the first step in preparing your Study Interview. After you are done with the setup of the study, you can move to planning the interviews.
Freeform Interview
This interview type is all about not being strictly connected to one of the study types. It is best suited for conducting exploratory research and just talking to your participants. Another use can be if you want to combine multiple study approaches in one interview.
There is an option to include a custom link in your interview planning, which can be easily shared with the participants in the call. Since there is no study directly connected to this interview type, you will start the setup process with planning your interview right away.
Information
- Author Services
Initiatives
You are accessing a machine-readable page. In order to be human-readable, please install an RSS reader.
All articles published by MDPI are made immediately available worldwide under an open access license. No special permission is required to reuse all or part of the article published by MDPI, including figures and tables. For articles published under an open access Creative Common CC BY license, any part of the article may be reused without permission provided that the original article is clearly cited. For more information, please refer to https://www.mdpi.com/openaccess .
Feature papers represent the most advanced research with significant potential for high impact in the field. A Feature Paper should be a substantial original Article that involves several techniques or approaches, provides an outlook for future research directions and describes possible research applications.
Feature papers are submitted upon individual invitation or recommendation by the scientific editors and must receive positive feedback from the reviewers.
Editor’s Choice articles are based on recommendations by the scientific editors of MDPI journals from around the world. Editors select a small number of articles recently published in the journal that they believe will be particularly interesting to readers, or important in the respective research area. The aim is to provide a snapshot of some of the most exciting work published in the various research areas of the journal.
Original Submission Date Received: .
- Active Journals
- Find a Journal
- Proceedings Series
- For Authors
- For Reviewers
- For Editors
- For Librarians
- For Publishers
- For Societies
- For Conference Organizers
- Open Access Policy
- Institutional Open Access Program
- Special Issues Guidelines
- Editorial Process
- Research and Publication Ethics
- Article Processing Charges
- Testimonials
- Preprints.org
- SciProfiles
- Encyclopedia
Article Menu

- Subscribe SciFeed
- Recommended Articles
- Google Scholar
- on Google Scholar
- Table of Contents
Find support for a specific problem in the support section of our website.
Please let us know what you think of our products and services.
Visit our dedicated information section to learn more about MDPI.
JSmol Viewer
The implementation and barriers of green recruitment: a qualitative study on green human resource management.

1. Introduction
2. literature review, 2.1. green human resource management (ghrm).
| GHRM Practices | Definition |
|---|---|
| Green Recruitment and Selection | Select candidates who demonstrate a commitment and sensitivity to environmental issues, and who are willing to contribute to these through internal or external recruitment processes. |
| Green Training | Establish a learning system focused on environmental issues to enhance employees’ awareness and skills for environmental responsibilities in their roles. |
| Green Performance Management | Evaluate employees’ environmental performance through the operational process to assess their contribution to the organisation’s green goals. |
| Green Reward | Monetary and non-monetary incentives to employees whose attitudes or behaviours help the firm’s environmental management. |
| Green Involvement | Employees are offered the chance to take part in environmental management initiatives which encompass participation, and fostering a culture of support and knowledge, all aimed at enhancing the employee’s dedication toward the organisation’s environmental management. |
2.2. Green Recruitment and Selection (GRS)
2.3. barriers for ghrm implementation.
| Barrier | Reference |
|---|---|
| 1 Lack of engagement in green issues (both organisational and individual) | Jackson & Seo, 2010 [ ]; Harvey et al., 2013 [ ]; Sobaih, 2019 [ ]; Tanveer et al., 2023 [ ] |
| 2 Financial Pressure | Sapna & Gupta, 2021 [ ]; Tweneboa Kodua et al., 2022 [ ]; Tanveer et al., 2023) [ ] |
| 3 Ambiguity of GHRM policy and the effectiveness measurement | Agarwal & Kapoor, 2022 [ ]; Tweneboa Kodua et al., 2022 [ ]; Fayyazi et al., 2015 [ ] |
| 4 Emotional Exhaustion | Yuan et al., 2023 [ ] |
2.4. Research Gaps
3. research methods, 4. results and discussion, 4.1. paperless recruitment, 4.2. green candidate recruitment, 5. discussion, 6. conclusions and recommendations, 7. limitation and future direction, author contributions, institutional review board statement, informed consent statement, data availability statement, conflicts of interest.
- Alvarado, R.; Toledo, E. Environmental degradation and economic growth: Evidence for a developing country. Environ. Dev. Sustain. 2016 , 19 , 1205–1218. [ Google Scholar ] [ CrossRef ]
- Saeed, B.B.; Afsar, B.; Hafeez, S.; Khan, I.; Tahir, M.; Afridi, M.A. Promoting employee’s proenvironmental behavior through green human resource management practices. Corp. Soc. Responsib. Environ. Manag. 2019 , 26 , 424–438. [ Google Scholar ] [ CrossRef ]
- Shil, P. Evolution and future of environmental marketing. Asia Pac. J. Mark. Manag. Rev. 2012 , 1 , 74–81. [ Google Scholar ]
- Atif, M.; Alam, M.S.; Islam, M.S. Firm-level energy and carbon performance: Does sustainable investment matter? Bus. Strategy Environ. 2022 , 32 , 2275–2295. [ Google Scholar ] [ CrossRef ]
- Hunt, C.B.; Auster, E.R. Proactive environmental management: Avoiding the toxic trap. MIT Sloan Manag. Rev. 1990 , 31 , 7. [ Google Scholar ]
- Borri, F.; Boccaletti, G. From total quality management to total quality environmental management. TQM Mag. 1995 , 7 , 38–42. [ Google Scholar ] [ CrossRef ]
- Boiral, O. Global warming: Should companies adopt a proactive strategy? Long Range Plan. 2006 , 39 , 315–330. [ Google Scholar ] [ CrossRef ]
- Moon, S.-G.; DeLeon, P. Contexts and corporate voluntary environmental behaviors: Examining the EPA’s green lights voluntary program. Organ. Environ. 2007 , 20 , 480–496. [ Google Scholar ] [ CrossRef ]
- Teixeira, A.A.; Jabbour, C.J.C.; Jabbour, A.B.L.d.S. Relationship between green management and environmental training in companies located in Brazil: A theoretical framework and case studies. Int. J. Prod. Econ. 2012 , 140 , 318–329. [ Google Scholar ] [ CrossRef ]
- Wehrmeyer, W. Greening People: Human Resources and Environmental Management ; Taylor & Francis Group: Saltaire, UK, 1996. [ Google Scholar ]
- Munawar, S.; Yousaf, D.H.Q.; Ahmed, M.; Rehman, D.S. Effects of green human resource management on green innovation through green human capital, environmental knowledge, and managerial environmental concern. J. Hosp. Tour. Manag. 2022 , 52 , 141–150. [ Google Scholar ] [ CrossRef ]
- Clair, J.A.; Milliman, J.; Whelan, K.S. Toward an environmentally sensitive ecophilosophy for business management. Ind. Environ. Crisis Q. 1996 , 9 , 289–326. [ Google Scholar ] [ CrossRef ]
- Ahmad, S.; Nisar, T. Green Human Resource Management: Policies and practices. Cogent Bus. Manag. 2015 , 2 , 1030817. [ Google Scholar ] [ CrossRef ]
- Jackson, S.E.; Renwick, D.W.; Jabbour, C.J.; Muller-Camen, M. State-of-the-art and future directions for green human resource management: Introduction to the special issue. Ger. J. Hum. Resour. Manag. 2011 , 25 , 99–116. [ Google Scholar ] [ CrossRef ]
- Paulet, R.; Holland, P.; Morgan, D. A meta-review of 10 years of green human resource management: Is Green HRM headed towards a roadblock or a revitalisation? Asia Pac. J. Hum. Resour. 2021 , 59 , 159–183. [ Google Scholar ] [ CrossRef ]
- Renwick, D.; Redman, T.; Maguire, S. Green HRM: A review, process model, and research agenda. Univ. Sheff. Manag. Sch. Discuss. Pap. 2008 , 1 , 1–46. [ Google Scholar ]
- Tang, G.; Chen, Y.; Jiang, Y.; Paillé, P.; Jia, J. Green human resource management practices: Scale development and validity. Asia Pac. J. Hum. Resour. 2018 , 56 , 31–55. [ Google Scholar ] [ CrossRef ]
- Ogiemwonyi, O.; Alam, M.N.; Alotaibi, H.S. Connecting green HRM practices to pro-environmental behavior through green human capital in the hospitality sector. Bus. Strategy Dev. 2023 , 6 , 1053–1071. [ Google Scholar ] [ CrossRef ]
- Shoaib, M.; Abbas, Z.; Yousaf, M.; Zámečník, R.; Ahmed, J.; Saqib, S. The role of GHRM practices towards organizational commitment: A mediation analysis of green human capital. Cogent Bus. Manag. 2021 , 8 , 1870798. [ Google Scholar ] [ CrossRef ]
- Pham, D.D.T.; Paillé, P. Green recruitment and selection: An insight into green patterns. Int. J. Manpow. 2019 , 41 , 258–272. [ Google Scholar ] [ CrossRef ]
- Renwick, D.W.; Redman, T.; Maguire, S. Green human resource management: A review and research agenda. Int. J. Manag. Rev. 2013 , 15 , 1–14. [ Google Scholar ] [ CrossRef ]
- Sapna; Gupta, A. Implementation of Green Human Resource Management Practices: Barriers and Solutions. J. Sci. Res. 2021 , 65 , 71–77. [ Google Scholar ] [ CrossRef ]
- Agarwal, A.; Kapoor, K. Analysis of barriers in green human resource implementation for enhancing organizational sustainability: A DEMATEL approach. Transnatl. Corp. Rev. 2022 , 15 , 1–15. [ Google Scholar ] [ CrossRef ]
- Fawehinmi, O.; Yusliza, M.Y.; Mohamad, Z.; Noor Faezah, J.; Muhammad, Z. Assessing the green behaviour of academics. Int. J. Manpow. 2020 , 41 , 879–900. [ Google Scholar ] [ CrossRef ]
- Dumont, J.; Shen, J.; Deng, X. Effects of Green HRM Practices on Employee Workplace Green Behavior: The Role of Psychological Green Climate and Employee Green Values. Hum. Resour. Manag. 2017 , 56 , 613–627. [ Google Scholar ] [ CrossRef ]
- Rayner, J.; Morgan, D. An empirical study of ‘green’ workplace behaviours: Ability, motivation and opportunity. Asia Pac. J. Hum. Resour. 2018 , 56 , 56–78. [ Google Scholar ] [ CrossRef ]
- Paillé, P.; Valéau, P.; Renwick, D.W. Leveraging green human resource practices to achieve environmental sustainability. J. Clean. Prod. 2020 , 260 , 121137. [ Google Scholar ] [ CrossRef ]
- Yusiana, R.; Widodo, A.; Hidayat, A.M.; Oktaviani, P.K. Green brand effects on green purchase intention (life restaurant never ended). Dinasti Int. J. Manag. Sci. 2020 , 1 , 762–768. [ Google Scholar ] [ CrossRef ]
- Phillips, L. Go green to gain the edge over rivals. People Manag. 2007 , 23 , 1–9. [ Google Scholar ]
- Grolleau, G.; Mzoughi, N.; Pekovic, S. Green not (only) for profit: An empirical examination of the effect of environmental-related standards on employees’ recruitment. Resour. Energy Econ. 2012 , 34 , 74–92. [ Google Scholar ] [ CrossRef ]
- Sinaga, S.A.; Nawangsari, L.C. The effect of green recruitment, green training on employee performance in pt tru using organization citizenship for environment as mediation variable. Dinasti Int. J. Manag. Sci. 2019 , 1 , 204–216. [ Google Scholar ] [ CrossRef ]
- Pham, N.T.; Hoang, H.T.; Phan, Q.P.T. Green human resource management: A comprehensive review and future research agenda. Int. J. Manpow. 2019 , 41 , 845–878. [ Google Scholar ] [ CrossRef ]
- Appelbaum, E.; Bailey, T.; Berg, P.; Kalleberg, A.L. Manufacturing Advantage: Why High-Performance Work Systems Pay Off ; Cornell University Press: Ithaca, NY, USA, 2000. [ Google Scholar ]
- Saini, P.; Shukla, K. Green recruitment: A new tool of cost cutting (conceptual study). Int. J. Sci. Innov. Res. 2016 , 4 , 195–198. [ Google Scholar ]
- Castellini, V. Environmentalism put to work: Ideologies of green recruitment in Toronto. Geoforum 2019 , 104 , 63–70. [ Google Scholar ] [ CrossRef ]
- Nyathi, M.; Kekwaletswe, R. Electronic human resource management (e-HRM) configuration for organizational success: Inclusion of employee outcomes as contextual variables. J. Organ. Eff. People Perform. 2023 , 11 , 196–212. [ Google Scholar ] [ CrossRef ]
- Bos-Nehles, A.; Townsend, K.; Cafferkey, K.; Trullen, J. Examining the Ability, Motivation and Opportunity (AMO) framework in HRM research: Conceptualization, measurement and interactions. Int. J. Manag. Rev. 2023 , 25 , 725–739. [ Google Scholar ] [ CrossRef ]
- Del Brío, J.Á.; Fernandez, E.; Junquera, B. Management and employee involvement in achieving an environmental action-based competitive advantage: An empirical study. The Int. J. Hum. Resour. Manag. 2007 , 18 , 491–522. [ Google Scholar ] [ CrossRef ]
- Qalati, S.A.; Barbosa, B.; Ibrahim, B. Factors influencing employees’ eco-friendly innovation capabilities and behavior: The role of green culture and employees’ motivations. Environ. Dev. Sustain. 2023 , 10 , 1–22. [ Google Scholar ] [ CrossRef ]
- Abiwu, L.; Nunoo, G.N. Green Recruitment Practices. In Human Resource Management Practices for Promoting Sustainability ; IGI Global: Hershey, PA, USA, 2021; pp. 73–93. [ Google Scholar ]
- Jackson, S.E.; Seo, J. The greening of strategic HRM scholarship. Organ. Manag. J. 2010 , 7 , 278–290. [ Google Scholar ] [ CrossRef ]
- Harvey, G.; Williams, K.; Probert, J. Greeningthe airline pilot: HRM and the green performance of airlines in the UK. Int. J. Hum. Resour. Manag. 2013 , 24 , 152–166. [ Google Scholar ] [ CrossRef ]
- Sathasivam, K.; Che Hashim, R.; Abu Bakar, R. Automobile industry managers’ views on their roles in environmental sustainability: A qualitative study. Manag. Environ. Qual. Int. J. 2021 , 32 , 844–862. [ Google Scholar ] [ CrossRef ]
- Sathasivam, K.; Abu Bakar, R.; Che Hashim, R. Embracing organisational environmental sustainability: Experiences in green human resource management. Bus. Strategy Dev. 2021 , 4 , 123–135. [ Google Scholar ] [ CrossRef ]
- Tuan, L.T. Promoting employee green behavior in the Chinese and Vietnamese hospitality contexts: The roles of green human resource management practices and responsible leadership. Int. J. Hosp. Manag. 2022 , 105 , 103253. [ Google Scholar ] [ CrossRef ]
- Sobaih, A. Green Human Resource Management in Egyptian Hotels: Practices and Barriers. Int. Acad. J. Fac. Tour. Hotel Manag. 2019 , 5 , 127–148. [ Google Scholar ] [ CrossRef ]
- Tweneboa Kodua, L.; Xiao, Y.; Adjei, N.O.; Asante, D.; Ofosu, B.O.; Amankona, D. Barriers to green human resources management (GHRM) implementation in developing countries. Evidence from Ghana. J. Clean. Prod. 2022 , 340 , 130671. [ Google Scholar ] [ CrossRef ]
- Jafri, S. Green HR practices: An empirical study of certain automobile organizations of India. Hum. Resour. Manag. 2012 , 42 , 6193–6198. [ Google Scholar ]
- Cho, S.; Chung, C.; Young, J. Study on the Relationship between CSR and Financial Performance. Sustainability 2019 , 11 , 343. [ Google Scholar ] [ CrossRef ]
- Bombiak, E. Barierrs to implementing the concept of green human resource management: The case of Poland. Eur. Res. Stud. J. 2020 , 23 , 66–81. [ Google Scholar ] [ CrossRef ]
- Fayyazi, M.; Shahbazmoradi, S.; Afshar, Z.; Shahbazmoradi, M.R. Investigating the barriers of the green human resource management implementation in oil industry. Manag. Sci. Lett. 2015 , 5 , 101–108. [ Google Scholar ] [ CrossRef ]
- Yuan, Y.; Ren, S.; Tang, G.; Ji, H.; Cooke, F.L.; Wang, Z. How green human resource management affects employee voluntary workplace green behaviour: An integrated model. Hum. Resour. Manag. J. 2023 , 34 , 91–121. [ Google Scholar ] [ CrossRef ]
- Tanveer, M.I.; Yusliza, M.Y.; Fawehinmi, O. Green HRM and hospitality industry: Challenges and barriers in adopting environmentally friendly practices. J. Hosp. Tour. Insights 2023 , 7 , 121–141. [ Google Scholar ] [ CrossRef ]
- Amjad, F.; Abbas, W.; Zia-Ur-Rehman, M.; Baig, S.A.; Hashim, M.; Khan, A.; Rehman, H.U. Effect of green human resource management practices on organizational sustainability: The mediating role of environmental and employee performance. Environ. Sci. Pollut. Res. Int. 2021 , 28 , 28191–28206. [ Google Scholar ] [ CrossRef ]
- Leidner, S.; Baden, D.; Ashleigh, M.J. Green (environmental) HRM: Aligning ideals with appropriate practices. Pers. Rev. 2019 , 48 , 1169–1185. [ Google Scholar ] [ CrossRef ]
- Giorgi, A. The Descriptive Phenomenological Method in Psychology: A Modified Husserlian Approach ; Duquesne University Press: Pittsburgh, PA, USA, 2009. [ Google Scholar ]
- Denzin, N.K. The Qualitative Manifesto: A Call to Arms ; Routledge: London, UK, 2018. [ Google Scholar ]
- Creswell, J.W.; Creswell, J.D. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches ; Sage Publications: Newbury Park, CA, USA, 2017. [ Google Scholar ]
- Kallio, H.; Pietilä, A.M.; Johnson, M.; Kangasniemi, M. Systematic methodological review: Developing a framework for a qualitative semi-structured interview guide. J. Adv. Nurs. 2016 , 72 , 2954–2965. [ Google Scholar ] [ CrossRef ] [ PubMed ]
- Pham, N.T.; Tučková, Z.; Chiappetta Jabbour, C.J. Greening the hospitality industry: How do green human resource management practices influence organizational citizenship behavior in hotels? A mixed-methods study. Tour. Manag. 2019 , 72 , 386–399. [ Google Scholar ] [ CrossRef ]
- Islam, M.A.; Hunt, A.; Jantan, A.H.; Hashim, H.; Chong, C.W. Exploring challenges and solutions in applying green human resource management practices for the sustainable workplace in the ready-made garment industry in Bangladesh. Bus. Strategy Dev. 2019 , 3 , 332–343. [ Google Scholar ] [ CrossRef ]
- Aldawish, L.; Kasturiratne, D.; Lean, J.; Phillips, C.; Wang, J. An exploration of the Role of Culture in Social Media Advertising and Consumer Purchase Decisionin the Saudi Arabia Fashion Market: A Qualitative Study. Gulf J. Adv. Bus. Res. 2024 , 2 , 78–92. [ Google Scholar ]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006 , 3 , 77–101. [ Google Scholar ] [ CrossRef ]
- Renwick, D.W.S. Contemporary Developments in Green Human Resource Management Research: Towards Sustainability in Action? 1st ed.; Routledge: London, UK, 2018. [ Google Scholar ]
- Gilal, F.G.; Ashraf, Z.; Gilal, N.G.; Gilal, R.G.; Chaana, N.A. Promoting environmental performance through green human resource management practices in higher education institutions: A moderated mediation model. Corp. Soc. Responsib. Environ. Manag. 2019 , 26 , 1579–1590. [ Google Scholar ] [ CrossRef ]
Click here to enlarge figure
| No. | Firm Type | Industry Type | ROLE | Industry Category | Profit Oritented |
|---|---|---|---|---|---|
| 1 | Neighbor Community | Non-profit Organization | Leader of Community | Low Carbon Emission | Non For-Profit |
| 2 | Neighbor Community | Non-profit Organization | Leader of Community | ||
| 3 | Neighbor Community | Non-profit Organization | Leader of Community | ||
| 4 | Neighbor Community | Non-profit Organization | Leader of Community | ||
| 5 | Public Fund | Financial Institution | HR Manager | For profit | |
| 6 | Public Fund | Financial Institution | Fund Sales Manger | ||
| 7 | Investment Bank | Financial Institution | CEO | ||
| 8 | Investment Bank | Financial Institution | HR Manager | ||
| 9 | Commerical Bank | Financial Institution | HR Manager | ||
| 10 | Futures | Financial Institution | HR Manager | ||
| 11 | AI | Information Technology | Leader | ||
| 12 | Website Production | Information Technology | Owner | ||
| 13 | Oil | Energy | HR Manager | High Carbon Emission | |
| 14 | Oil | Energy | HR Manager | ||
| 15 | Gas | Energy | Training Manager | ||
| 16 | Chemical | Chemical industry | HR Manager | ||
| 17 | Restaurant | Food Industry | Owner | ||
| 18 | Restaurant | Food Industry | Owner | ||
| 19 | Hotel | Hotel Industry | HR Manager | ||
| 20 | Hotel | Hotel Industry | HR Manager |
| The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
Share and Cite
Wang, J.; Tang, L.; Zhang, T.; Phillips, C.; Aldawish, L.S. The Implementation and Barriers of Green Recruitment: A Qualitative Study on Green Human Resource Management. Businesses 2024 , 4 , 411-425. https://doi.org/10.3390/businesses4030025
Wang J, Tang L, Zhang T, Phillips C, Aldawish LS. The Implementation and Barriers of Green Recruitment: A Qualitative Study on Green Human Resource Management. Businesses . 2024; 4(3):411-425. https://doi.org/10.3390/businesses4030025
Wang, Jinghan, Lijun Tang, Tiancheng Zhang, Chris Phillips, and Lamis Sultan Aldawish. 2024. "The Implementation and Barriers of Green Recruitment: A Qualitative Study on Green Human Resource Management" Businesses 4, no. 3: 411-425. https://doi.org/10.3390/businesses4030025
Article Metrics
Article access statistics, further information, mdpi initiatives, follow mdpi.
Subscribe to receive issue release notifications and newsletters from MDPI journals
- Open access
- Published: 02 September 2024
Clinical supervisor’s experiences of peer group clinical supervision during COVID-19: a mixed methods study
- Owen Doody ORCID: orcid.org/0000-0002-3708-1647 1 ,
- Kathleen Markey ORCID: orcid.org/0000-0002-3024-0828 1 ,
- James Turner ORCID: orcid.org/0000-0002-8360-1420 2 ,
- Claire O. Donnell ORCID: orcid.org/0000-0003-2386-7048 1 &
- Louise Murphy ORCID: orcid.org/0000-0003-2381-3963 1
BMC Nursing volume 23 , Article number: 612 ( 2024 ) Cite this article
Metrics details
Providing positive and supportive environments for nurses and midwives working in ever-changing and complex healthcare services is paramount. Clinical supervision is one approach that nurtures and supports professional guidance, ethical practice, and personal development, which impacts positively on staff morale and standards of care delivery. In the context of this study, peer group clinical supervision provides allocated time to reflect and discuss care provided and facilitated by clinical supervisors who are at the same grade/level as the supervisees.
To explore the clinical supervisor’s experiences of peer group clinical supervision a mixed methods study design was utilised within Irish health services (midwifery, intellectual disability, general, mental health). The Manchester Clinical Supervision Scale was used to survey clinical supervisors ( n = 36) and semi-structured interviews ( n = 10) with clinical supervisors were conducted. Survey data were analysed through SPSS and interview data were analysed utilising content analysis. The qualitative and quantitative data’s reporting rigour was guided by the CROSS and SRQR guidelines.
Participants generally had a positive encounter when providing clinical supervision. They highly appreciated the value of clinical supervision and expressed a considerable degree of contentment with the supervision they provided to supervisees. The advantages of peer group clinical supervision encompass aspects related to self (such as confidence, leadership, personal development, and resilience), service and organisation (including a positive working environment, employee retention, and safety), and patient care (involving critical thinking and evaluation, patient safety, adherence to quality standards, and elevated levels of care).
There are many benefits of peer group clinical supervision at an individual, service, organisation, and patient level. Nevertheless, there is a need to address a lack of awareness and misconceptions surrounding clinical supervision to create an environment and culture conducive to realising its full potential. It is crucial that clinical supervision be accessible to nurses and midwives of all grades across all healthcare services, with national planning to address capacity and sustainability.
Peer Review reports
Within a dynamic healthcare system, nurses and midwives face growing demands, underscoring the necessity for ongoing personal and professional development. This is essential to improve the effectiveness and efficiency of care delivery for patients, families, and societies. Despite the increased emphasis on increasing the quality and safety of healthcare services and delivery, there is evidence highlighting declining standards of nursing and midwifery care [ 1 ]. The recent focus on re-affirming and re-committing to core values guiding nursing and midwifery practice is encouraging such as compassion, care and commitment [ 2 ], competence, communication, and courage [ 3 ]. However, imposing value statements in isolation is unlikely to change behaviours and greater consideration needs to be given to ways in which compassion, care, and commitment are nurtured and ultimately applied in daily practice. Furthermore, concerns have been raised about global staff shortages [ 4 ], the evidence suggesting several contributing factors such as poor workforce planning [ 5 ], job dissatisfaction [ 6 ], and healthcare migration [ 7 ]. Without adequate resources and staffing, compromising standards of care and threats to patient safety will be imminent therefore the importance of developing effective strategies for retaining competent registered nurses and midwives is paramount in today’s climate of increased staff shortages [ 4 ]. Clinical supervision serves as a means to facilitate these advancements and has been linked to heightened job satisfaction, enhanced staff retention, improved staff effectiveness, and effective clinical governance, by aiding in quality improvements, risk management, and heightened accountability [ 8 ].
Clinical supervision is a key component of professional practice and while the aim is largely known, there is no universally accepted definition of clinical supervision [ 8 ]. Clinical supervision is a structured process where clinicians are allowed protected time to reflect on their practice within a supportive environment and with the purpose of developing high-quality clinical care [ 9 ]. Recent literature published on clinical supervision [ 8 , 9 , 10 , 11 , 12 , 13 , 14 , 15 , 16 ] highlights the advantages and merits of clinical supervision. However, there are challenges also identified such as a lack of consensus regarding the meaning and goal, implementation issues, variations in approaches in its operationalisation, and an absence of research evidence on its effectiveness. Duration and experience in clinical supervision link to positive benefits [ 8 ], but there is little evidence of how clinical supervision altered individual behaviours and practices. This is reinforced by Kuhne et al., [ 15 ] who emphasise that satisfaction rather than effectiveness is more commonly examined. It is crucial to emphasise that reviews have pinpointed that clinical supervision lowers the risks of adverse patient outcomes [ 9 ] and demonstrates enhancements in the execution of certain care processes. Peer group clinical supervision is a form of clinical supervision whereby two or more practitioners engage in a supervision or consultation process to improve their professional practice [ 17 ]. There is limited evidence regarding peer group clinical supervision and research on the experiences of peer clinical supervision and stakeholders is needed [ 13 ]. In Ireland, peer group clinical supervision has been recommended and guidelines have been developed [ 18 ]. In the Irish context, peer clinical supervision is where both clinical supervisees and clinical supervisors are peers at the same level/grade. However, greater evidence is required to inform future decisions on the implementation of peer group clinical supervision and the purpose of this study is to explore clinical supervisors’ experiences of peer group clinical supervision. As the focus is on peer group supervisors and utilising mixed methods the experiences of the other stakeholders were investigated and reported separately.
A mixed methods approach was used (survey and semi-structured interviews) to capture clinical supervisor’s experiences of clinical supervision. The study adhered to the Consensus-Based Checklist for Reporting of Survey Studies guidelines [ 19 ] (Supplementary File S1 ) and Standards for Reporting Qualitative Research guidelines [ 20 ] (Supplementary File S2 ).
Participants
This study was conducted with participants who successfully completed a professionally credited award: clinical supervision module run by a university in Ireland (74 clinical supervisors across 5 programmes over 3 years). The specific selection criteria for participants were that they were registered nurses/midwives delivering peer group clinical supervision within the West region of Ireland. The specific exclusion criteria were as follows: (1) nurses and midwives who haven’t finished the clinical supervision module at the University, (2) newly appointed peer group clinical supervisors who have yet to establish their groups and initiate the delivery of peer group clinical supervision.
Measures and procedures
The Manchester Clinical Supervision Scale-26 was used to survey participants in February/March 2022 and measure the peer group clinical supervisors’ overall experiences of facilitating peer group clinical supervision. The Manchester Clinical Supervision Scale-26 is a validated 26-item self-report questionnaire with a Likert-type (1–5) scale ranging from strongly disagree (1) to strongly agree (5) [ 21 ]. The Manchester Clinical Supervision Scale-26 measures the efficiency of and satisfaction with supervision, to investigate the skills acquisition aspect of clinical supervision and its effect on the quality of clinical care [ 21 ]. The instrument consists of two main sections to measure three (normative, restorative, and formative) dimensions of clinical supervision utilising six sub-scales: (1) trust and rapport, (2) supervisor advice/support, (3) improved care/skills, (4) importance/value of clinical supervision, (5) finding time, (6) personal issues/reflections and a total score for the Manchester Clinical Supervision Scale-26 is also calculated. Section two consisted of the demographic section of the questionnaire and was tailored to include eight demographic questions concerning the supervisor’s demographics, supervisee characteristics, and characteristics of clinical supervision sessions. There were also two open field questions on the Manchester Clinical Supervision Scale-26 (model of clinical supervision used and any other comments about experience of peer group clinical supervision). The main question about participants’ experiences with peer clinical supervision was “What was your experience of peer clinical supervision?” This was gathered through individual semi-structured interviews lasting between 20 and 45 min, in March/April 2022 (Supplementary file 3 ).
Ethical considerations
Health service institutional review boards of two University hospitals approved this study (Ref: 091/19 and Ref: C.A. 2199). Participants were recruited after receiving a full explanation of the study’s purpose and procedure and all relevant information. Participants were aware of potential risks and benefits and could withdraw from the study, or the survey could be stopped at any time. Informed consent was recorded, and participant identities were protected by using a pseudonym to protect anonymity.
Data analysis method
Survey data was analysed using the data analysis software package Statistical Package for the Social Sciences, version 26 (SPSS Inc., Chicago, Il, USA). Descriptive analysis was undertaken to summarise responses to all items and categorical variables (nominal and ordinal) were analysed using frequencies to detail the number and percentage of responses to each question. Scores on the Manchester Clinical Supervision Scale-26 were reverse scored for 9 items (Q1-Q6, Q8, Q20,21) and total scores for each of the six sub-scales were calculated by adding the scores for each item. Raw scores for the individual sub-scales varied in range from 0 to 20 and these raw scores were then converted to percentages which were used in addition to the raw scores for each sub-scale to describe and summarise the results of the Manchester Clinical Supervision Scale-26. Cronbach’s alpha coefficient was undertaken with the 26 questions included within the Manchester Clinical Supervision Scale-26 and more importantly with each of the dimensions in the Manchester Clinical Supervision Scale-26. The open-ended questions on the Manchester Clinical Supervision Scale-26 and interviews were analysed using content analysis guided by Colorafi and Evans [ 22 ] and categories were generated using their eight steps, (1) creating a coding framework, (2) adding codes and memos, (3) applying the first level of coding, (4) categorising codes and applying the second level of coding, (5) revising and redefining the codes, (6) adding memos, (7) visualising data and (8) representing the data.
Research rigour
To ensure the validity and rigour of this study the researchers utilised the Manchester Clinical Supervision Scale-26 a recognised clinical supervision tool with good reliability and wide usage. Interviews were recorded, transcribed, and verified by four participants, data were collected until no new components appeared, data collection methods and analysis procedures were described, and the authors’ biases were minimised throughout the research process. The Manchester Clinical Supervision Scale-26 instrument internal consistency reliability was assessed which was overall good (α = 0.878) with individual subscale also good e.g., normative domain 0.765, restorative domain 0.864, and formative domain 0.900. Reporting rigour was demonstrated using the Consensus-Based Checklist for Reporting of Survey Studies guidelines [ 19 ] and Standards for Reporting Qualitative Research guidelines [ 20 ].
Quantitative data
Participant and clinical supervision characteristics.
Thirty-six of the fifty-two (69.2%) peer group clinical supervisors working across a particular region of Ireland responded to the Manchester Clinical Supervision Scale-26 survey online via Qualtrics. Table 1 identifies the demographics of the sample who were predominantly female (94.4%) with a mean age of 44.7 years (SD. 7.63).
Peer group clinical supervision session characteristics (Table 2 ) highlight over half of peer group clinical supervisors ( n = 20, 55.6%) had been delivering peer group clinical supervision for less than one year and were mainly delivered to female supervisees ( n = 28, 77.8%). Most peer group clinical supervision sessions took place monthly ( n = 32, 88.9%) for 31–60 min ( n = 27, 75%).
Manchester Clinical Supervision Scale-26 results
Participants generally viewed peer group clinical supervision as effective (Table 3 ), the total mean Manchester Clinical Supervision Scale-26 score among all peer group clinical supervisors was 76.47 (SD. 12.801) out of 104, Surpassing the clinical supervision threshold score of 73, which was established by the developers of the Manchester Clinical Supervision Scale-26 as the benchmark indicating proficient clinical supervision provision [ 21 ]. Of the three domains; normative, formative, and restorative, the restorative domain scored the highest (mean 28.56, SD. 6.67). The mean scores compare favourably to that of the Manchester Clinical Supervision Scale-26 benchmark data and suggest that the peer group clinical supervisors were satisfied with both the level of support, encouragement, and guidance they provided and the level of trust/rapport they had developed during the peer group clinical supervision sessions. 83.3% ( n = 30) of peer group clinical supervisors reported being either very satisfied ( n = 12, 33.3%) or moderately satisfied ( n = 18, 50%) with the peer group clinical supervision they currently delivered. Within the peer group clinical supervisor’s supervisee related issues ( n = 17, 47.2%), work environment-related issues ( n = 16, 44.4%), staff-related issues ( n = 15, 41.7%) were reported as the most frequent issues, with patient/client related issues being less frequent ( n = 8, 22.2%). The most identified model used to facilitate peer group clinical supervision was the Proctors model ( n = 8, 22.22%), which was followed by group ( n = 2, 5.55%), peer ( n = 2, 5.55%), and a combination of the seven-eyed model of clinical supervision and Proctors model ( n = 1, 2.77%) with some not sure what model they used ( n = 2, 5.553%) and 58.33% ( n = 21) did not report what model they used.
Survey open-ended question
‘Please enter any additional comments , which are related to your current experience of delivering Peer Group Clinical Supervision.’ There were 22 response comments to this question, which represented 61.1% of the 36 survey respondents, which were analysed using content analysis guided by Colorafi & Evans [ 22 ]. Three categories were generated. These included: personal value/benefit of peer group clinical supervision, challenges with facilitating peer group clinical supervision, and new to peer group clinical supervision.
The first category ‘personal value/benefit of peer group clinical supervision’ highlighted positive experiences of both receiving and providing peer group clinical supervision. Peer group clinical supervisors reported that they enjoyed the sessions and found them both worthwhile and beneficial for both the group and them as peer group clinical supervisors in terms of creating a trusted supportive group environment and motivation to develop. Peer group clinical supervision was highlighted as very important for the peer group clinical supervisors working lives and they hoped that there would be more uptake from all staff. One peer group clinical supervisor expressed that external clinical supervision was a ‘lifeline’ to shaping their supervisory journey to date.
The second category ‘challenges with facilitating peer group clinical supervision’, identified time constraints, lack of buy-in/support from management, staff shortages, lack of commitment by supervisees, and COVID-19 pandemic restrictions and related sick leave, as potential barriers to facilitating peer group clinical supervision. COVID-19 was perceived to have a negative impact on peer group clinical supervision sessions due to staff shortages, which resulted in difficulties for supervisees attending the sessions during work time. Peer group clinical supervisors felt that peer group clinical supervision was not supported by management and there was limited ‘buy-in’ at times. There was also a feeling expressed that peer group clinical supervision was in its infancy, as COVID-19 and its related restrictions impacted on this by either slowing down the process of commencing peer group clinical supervision in certain areas or having to move online. However, more recently improvements in managerial support and supervisee engagement with the peer group clinical supervision process are noted.
The final category ‘new to peer group clinical supervision’ highlighted that some peer group clinical supervisors were new to the process of providing peer group clinical supervision and some felt that this survey was not a true reflection of their experience of delivering peer group clinical supervision, as they were not fully established yet as clinical supervisors due to the impact of COVID-19. Peer group clinical supervisors identified that while they were new to providing peer group clinical supervision, they were enjoying it and that it was a learning curve for them.
Qualitative data
The qualitative phase explored peer group clinical supervisors’ ( n = 10) own experiences of preparation received and experiences of being a peer group clinical supervisor. Three themes were identified through data analysis, building the foundations, enacting engagement and actions, and realities (Table 4 ).
Building the foundations
This theme highlights the importance of prior knowledge, awareness, and training but also the recruitment process and education in preparing peer group clinical supervisors.
Knowledge and awareness
Participant’s prior knowledge and awareness of peer group clinical supervision was mixed with some reporting having little or no knowledge of clinical supervision.
I’m 20 years plus trained as a nurse , and I had no awareness of clinical supervision beforehand , I really hadn’t got a clue what all of this was about , so it was a very new concept to me (Bernie) .
Others were excited about peer group clinical supervision and while they could see the need they were aware that there may be limited awareness of the value and process of clinical supervision among peers.
I find that there’s great enthusiasm and passion for clinical supervision as it’s a great support mechanism for staff in practice , however , there’s a lack of awareness of clinical supervision (Jane) .
Recruitment
Some participants highlighted that the recruitment process to become a peer group clinical supervisor was vague in some organisations with an unclear and non-transparent process evident where people were chosen by the organisation’s management rather than self-selecting interested parties.
It was just the way the training was put to the people , they were kind of nominated and told they were going and there was a lot of upset over that , so they ended up in some not going at all (Ailbhe) .
In addition, the recruitment process was seen as top loaded where senior grades of staff were chosen, and this limited staff nurse grade opportunities where there was a clear need for peer group clinical supervisors and support.
We haven’t got down to the ground level like you know we’ve done the directors , we’ve done the CNM3s the CNM2s we are at the CNM1s , so we need to get down to the staff nurse level so the nurses at the direct frontline are left out and aren’t receiving supervision because we don’t have them trained (Bernie) .
Training and education
Participants valued the training and education provided but there was a clear sense of ‘imposter syndrome’ for some peer group clinical supervisors starting out. Participants questioned their qualifications, training duration, and confidence to undertake the role of peer group clinical supervisor.
Because it is group supervision and I know that you know they say that we are qualified to do supervision and you know we’re now qualified clinical supervisors but I’m not sure that a three-month module qualifies you to be at the top of your game (Maria) .
Participants when engaged in the peer group clinical supervisor educational programme did find it beneficial and the true benefit was the actual re-engagement in education and published evidence along with the mix of nursing and midwifery practice areas.
I found it very beneficial , I mean I hadn’t been engaged in education here in a while , so it was great to be back in that field and you know with the literature that’s big (Claire) .
Enacting engagement and actions
This theme highlights the importance of forming the groups, getting a clear message out, setting the scene, and grounding the group.
Forming the groups
Recruitment for the group was of key importance to the peer group clinical supervisor and they all sent out a general invitation to form their group. Some supervisors used invitation letters or posters in addition to a general email and this was effective in recruiting supervisees.
You’re reaching out to people , I linked in with the ADoN and I put together a poster and circulated that I wasn’t ‘cherry picking , and I set up a meeting through Webex so people could get a sense of what it was if they were on the fence about it or unsure if it was for them (Karen) .
In forming the peer clinical supervision groups consideration needs to be given to the actual number of supervisees and participants reported four to six supervisees as ideal but that number can alter due to attendance.
The ideal is having five or six consistent people and that they all come on board and that you get the dynamics of the group and everything working (Claire) .
Getting a clear message out
Within the recruitment process, it was evident that there was a limited and often misguided understanding or perception of peer group clinical supervision.
Greater awareness of what actually clinical supervision is , people misjudge it as a supervision where someone is appraising you , when in fact it is more of a support mechanism , I think peer support is the key element that needs to be brought out (Jane) .
Given the lack of clarity and understanding regarding peer group clinical supervision, the participants felt strongly that further clarity is needed and that the focus needs to be on the support it offers to self, practice, and the profession.
Clinical supervision to me is clinical leadership (Jane) .
Setting the scene and grounding the group
In the initial phase of the group coming together the aspect of setting the scene and grounding the group was seen as important. A key aspect of this process was establishing the ground rules which not only set the boundaries and gave structure but also ensured the adoption of principles of trust, confidentiality, and safety.
We start with the ground rules , they give us structure it’s our contract setting out the commitment the expectation for us all , and the confidentiality as that’s so important to the trust and safety and building the relationships (Brid) .
Awareness of group dynamics is important in this process along with awareness of the group members (supervisees) as to their role and expectations.
I reiterate the role of each person in relation to confidentiality and the relationship that they would have with each other within the group and the group is very much aware that it is based on respect for each person’s point of view people may have a fear of contributing to the group and setting the ground rules is important (Jane) .
To ground the group, peer group clinical supervisors saw the importance of being present and allowing oneself to be in the room. This was evident in the time allocated at the start of each session to allow ‘grounding’ to occur in the form of techniques such as a short meditation, relaxation, or deep breathing.
At the start , I do a bit of relaxation and deep breathing , and I saw that with our own external supervisor how she settled us into place so very much about connecting with your body and you’ve arrived , then always come in with the contract in my first sentence , remember today you know we’re in a confidential space , of course , you can take away information , but the only information you will take from today is your own information and then the respect aspect (Mary Rose) .
This settling in and grounding was seen as necessary for people to feel comfortable and engage in the peer group clinical supervision process where they could focus, be open, converse, and be aware of their role and the role of peer group clinical supervision.
People have to be open, open about their practice and be willing to learn and this can only occur by sharing, clinical supervision gives us the space to do it in a space where we know we will be respected, and we can trust (Claire) .
This theme highlights the importance of the peer group clinical supervisors’ past experiences, delivering peer group clinical supervision sessions, responding to COVID-19, personal and professional development, and future opportunities.
Past experiences
Past experiences of peer group clinical supervisors were not always positive and for one participant this related to the lack of ground rules or focus of the sessions and the fact it was facilitated by a non-nurse.
In the past , I suppose I would have found it very frustrating as a participant because I just found that it was going round in circles , people moaning and you know it wasn’t very solution focused so I came from my situation where I was very frustrated with clinical supervision , it was facilitated by somebody that was non-nursing then it wasn’t very , there wasn’t the ground rules , it was very loose (Caroline) .
However, many did not have prior experience of peer group clinical supervision. Nonetheless, through the education and preparation received, there was a sense of commitment to embrace the concept, practice, and philosophy.
I did not really have any exposure or really much information on clinical supervision , but it has opened my eyes , and as one might say I am now a believer (Brid) .
Delivering peer group clinical supervision
In delivering peer group clinical supervision, participants felt supervisees were wary, as they did not know what peer group clinical supervision was, and they had focused more on the word supervision which was misleading to them. Nonetheless, the process was challenging, and buy-in was questioned at an individual and managerial level.
Buy-in wasn’t great I think now of course people will blame the pandemic , but this all happened before the pandemic , there didn’t seem to be you know , the same support from management that I would have expected so I kind of understood it in a way because then there wasn’t the same real respect from the practitioners either (Mary Rose) .
From the peer group clinical supervisor’s perspective, they were all novices in delivering/facilitating peer group clinical supervision sessions, and the support of the external clinical supervisors, and their own peer group clinical supervision sessions were invaluable along with a clinical supervision model.
Having supervision myself was key and something that is vital and needed , we all need to look at our practice and how we work it’s no good just facilitating others without being part of the process yourself but for me I would say the three principles of clinical supervision , you know the normative , formative and restorative , I keep hammering that home and bring that in regularly and revisit the contract and I have to do that often you know (Claire) .
All peer group clinical supervisors commented on the preparation for their peer group clinical supervision sessions and the importance of them having the right frame of mind and that often they needed to read over their course work and published evidence.
I want everybody to have a shared voice and you know that if one person , there is something that somebody feels very strongly and wants to talk about it that they e-mail in advance like we don’t have a set agenda but that’s agreed from the participant at the start (Caroline) .
To assist this, the peer group clinical supervisors noted the importance of their own peer group clinical supervision, the support of their peers, and external clinical supervisors. This preparation in an unpredictable situation can be difficult but drawing on one’s experience and the experience within the group can assist in navigating beyond unexpected situations.
I utilise the models of clinical supervision and this helps guide me , I am more of a facilitator of the group we are experts in our own area and our own role but you can only be an expert if you take the time to examine your practice and how you operate in your role (Brid) .
All clinical supervisors noted that the early sessions can be superficial, and the focus can be on other practice or management issues, but as time moves on and people become more engaged and involved it becomes easier as their understanding of supervision becomes clearer. In addition, there may be hesitancy and people may have difficulty opening up with certain people in the group and this is a reality that can put people off.
Initially there was so much managerial bashing and I think through supervision , I began to kind of think , I need the pillars of supervision , the governance , bringing more knowledge and it shifted everything in the room , trying to marry it with all the tensions that people have (Mary Rose) .
For some clinical supervisors, there were expected and unexpected challenges for them as clinical supervisors in terms of the discussions veering off course and expectations of their own ability.
The other big challenge is when they go off , how do you bring him back , you know when they veer off and you’re expected to be a peer , but you have to try and recoil that you have to get the balance with that right (Mary Rose) .
While peer group clinical supervision is accepted and seen as a valuable process by the peer group clinical supervisors, facilitating peer group supervision with people known to you can be difficult and may affect the process.
I’d love to supervise a group where I actually don’t know the people , I don’t know the dynamics within the group , and I’d love to see what it would be like in a group (Bernie) .
Of concern to clinical supervisors was the aspect of non-attendance and while there may be valid reasons such as COVID-19 the absence of a supervisee for several sessions can affect the group dynamics, especially if the supervisee has only engaged with early group sessions.
One of the ones that couldn’t attend because of COVID and whatever , but she’s coming to the next one and I just feel there’s a lot of issues in her area and I suppose I’m mindful that I don’t want that sort of thing to seep in , so I suppose it’s just for me just to keep reiterating the ground rules and the boundaries , that’s something I just have to manage as a facilitator , but what if they don’t attend how far will the group have progressed before she attends (Caroline) .
Responding to COVID-19
The advent of COVID-19 forced peer group clinical supervisors to find alternative means of providing peer group clinical supervision sessions which saw the move from face-to-face to online sessions. The online transition was seen as seamless for many established groups while others struggled to deliver sessions.
With COVID we did online for us it was fine because we were already formed (Corina) .
While the transition may have been positive many clinical supervisors came across issues because they were using an online format that would not be present in the face-to-face session.
We did have a session where somebody was in the main office and they have a really loud booming voice and they were saying stuff that was not appropriate to say outside of clinical supervision and I was like are you in the office can you lower it down a bit can you put your headphones on (Maria) .
However, two peer group clinical supervisors ceased or hasted the progress of rolling out peer group clinical supervision sessions mainly due to redeployment and staff availability.
With COVID it just had to be canceled here , it’s just the whole thing was canceled so it was very , very difficult for people (Mary Rose) .
It was clear from clinical supervisors that online sessions were appropriate but that they felt they were only appropriate for existing established groups that have had the opportunity to build relationships, develop trust, embed the ground rules, and create the space for open communication and once established a combined approach would be appropriate.
Since we weren’t as established as a group , not everybody knew each other it would be difficult to establish that so we would hold off/reschedule , obviously COVID is a major one but also I suppose if you have an established group now , and again , you could go to a remote one , but I felt like since we weren’t established as a group it would be difficult to develop it in that way (Karen) .
Within practice COVID-19 took priority and other aspects such as peer group clinical supervision moved lower down on the priority list for managers but not for the clinical supervisors even where redeployment occurred.
With COVID all the practical side , if one of the managers is dealing with an outbreak , they won’t be attending clinical supervision , because that has to be prioritised , whereas we’ve prioritised clinical supervision (Maria) .
The valuing of peer group clinical supervision was seen as important by clinical supervisors, and they saw it as particularly needed during COVID-19 as staff were dealing with many personal and professional issues.
During the height of COVID , we had to take a bit of a break for four months as things were so demanding at work for people but then I realised that clinical supervision was needed and started back up and they all wanted to come back (Brid) .
Having peer group clinical supervision during COVID-19 supported staff and enabled the group to form supportive relationships.
COVID has impacted over the last two years in every shape and they needed the supervision and the opportunity to have a safe supportive space and it gelled the group I think as we all were there for each other (Claire) .
While COVID-19 posed many challenges it also afforded clinical supervisors and supervisees the opportunity for change and to consider alternative means of running peer group clinical supervision sessions. This change resulted in online delivery and in reflecting on both forms of delivery (face-to-face and online) clinical supervisors saw the benefit in both. Face-to-face was seen as being needed to form the group and then the group could move online once the group was established with an occasional periodic face-to-face session to maintain motivation commitment and reinforce relationships and support.
Online formats can be effective if the group is already established or the group has gone through the storming and forming phase and the ground rules have been set and trust built , then I don’t see any problem with a blended online version of clinical supervision , and I think it will be effective (Jane) .
Personal and professional development
Growth and development were evident from peer group clinical supervisors’ experiences and this growth and development occurred at a personal, professional, and patient/client level. This development also produced an awakening and valuing of one’s passion for self and their profession.
I suppose clinical supervision is about development I can see a lot of development for me and my supervisees , you know personally and professionally , it’s the support really , clinical supervision can reinvigorate it’s very exciting and a great opportunity for nursing to support each other and in care provision (Claire) .
A key to the peer group clinical supervisor’s development was the aspect of transferable skills and the confidence they gained in fulfilling their role.
All of these skills that you learn are transferable and I am a better manager because of clinical supervision (Maria) .
The confidence and skills gained translated into the clinical supervisor’s own practice as a clinical practitioner and clinical supervisor but they were also realistic in predicting the impact on others.
I have empowered my staff , I empower them to use their voice and I give my supervisees a voice and hope they take that with them (Corina) .
Fundamental to the development process was the impact on care itself and while this cannot always be measured or identified, the clinical supervisors could see that care and support of the individual practitioner (supervisee) translated into better care for the patient/client.
Care is only as good as the person delivering it and what they know , how they function and what energy and passion they have , and clinical supervision gives the person support to begin to understand their practice and how and why they do things in a certain way and when they do that they can begin to question and even change their way of doing something (Brid) .
Future opportunities
Based on the clinical supervisor’s experiences there was a clear need identified regarding valuing and embedded peer group clinical supervision within nursing/midwifery practice.
There has to be an emphasis placed on supervision it needs to be part of the fabric of a service and valued by all in that service , we should be asking why is it not available if it’s not there but there is some work first on promoting it and people knowing what it actually is and address the misconceptions (Claire) .
While such valuing and buy-in are important, it is not to say that all staff need to have peer group clinical supervision so as to allow for personal choice. In addition, to value peer group clinical supervision it needs to be evident across all staffing grades and one could question where the best starting point is.
While we should not mandate that all staff do clinical supervision it should become embedded within practice more and I suppose really to become part of our custom and practice and be across all levels of staff (Brid) .
When peer group clinical supervision is embedded within practice then it should be custom and practice, where it is included in all staff orientations and is nationally driven.
I suppose we need to be driving it forward at the coal face at induction , at orientation and any development for the future will have to be driven by the NMPDUs or nationally (Ailbhe) .
A formalised process needs to address the release of peer group clinical supervisors but also the necessity to consider the number of peer group clinical supervisors at a particular grade.
The issue is release and the timeframe as they have a group but they also have their external supervision so you have to really work out how much time you’re talking about (Maria) .
Vital within the process of peer group clinical supervision is receiving peer group clinical supervision and peer support and this needs to underpin good peer group clinical supervision practice.
Receiving peer group supervision helps me , there are times where I would doubt myself , it’s good to have the other group that I can go to and put it out there to my own group and say , look at this , this is what we did , or this is what came up and this is how (Bernie) .
For future roll out to staff nurse/midwife grade resourcing needs to be considered as peer group clinical supervisors who were managers could see the impact of having several peer group clinical supervisors in their practice area may have on care delivery.
Facilitating groups is an issue and needs to be looked at in terms of the bigger picture because while I might be able to do a second group the question is how I would be supported and released to do so (Maria) .
While there was ambiguity regarding peer group clinical supervision there was an awareness of other disciplines availing of peer group clinical supervision, raising questions about the equality of supports available for all disciplines.
I always heard other disciplines like social workers would always have been very good saying I can’t meet you I have supervision that day and I used to think my God what’s this fabulous hour that these disciplines are getting and as a nursing staff it just wasn’t there and available (Bernie) .
To address this equity issue and the aspect of low numbers of certain grades an interdisciplinary approach within nursing and midwifery could be used or a broader interdisciplinary approach across all healthcare professionals. An interdisciplinary or across-services approach was seen as potentially fruitful.
I think the value of interprofessional or interdisciplinary learning is key it addresses problem-solving from different perspectives that mix within the group is important for cross-fertilisation and embedding the learning and developing the experience for each participant within the group (Jane) .
As we move beyond COVID-19 and into the future there is a need to actively promote peer group clinical supervision and this would clarify what peer group clinical supervision actually is, its uptake and stimulate interest.
I’d say it’s like promoting vaccinations if you could do a roadshow with people , I think that would be very beneficial , and to launch it , like you have a launch an official launch behind it (Mary Rose) .
The advantages of peer group clinical supervision highlighted in this study pertain to self-enhancement (confidence, leadership, personal development, resilience), organisational and service-related aspects (positive work environment, staff retention, safety), and professional patient care (critical thinking and evaluation, patient safety, adherence to quality standards, elevated care standards). These findings align with broader literature that acknowledges various areas, including self-confidence and facilitation [ 23 ], leadership [ 24 ], personal development [ 25 ], resilience [ 26 ], positive/supportive working environment [ 27 ], staff retention [ 28 ], sense of safety [ 29 ], critical thinking and evaluation [ 30 ], patient safety [ 31 ], quality standards [ 32 ] and increased standards of care [ 33 ].
In this study, peer group clinical supervision appeared to contribute to the alleviation of stress and anxiety. Participants recognised the significance of these sessions, where they could openly discuss and reflect on professional situations both emotionally and rationally. Central to these discussions was the creation of a safe, trustworthy, and collegial environment, aligning with evidence in the literature [ 34 ]. Clinical supervision provided a platform to share resources (information, knowledge, and skills) and address issues while offering mutual support [ 35 ]. The emergence of COVID-19 has stressed the significance of peer group clinical supervision and support for the nursing/midwifery workforce [ 36 ], highlighting the need to help nurses/midwifes preserve their well-being and participate in collaborative problem-solving. COVID-19 impacted and disrupted clinical supervision frequency, duration and access [ 37 ]. What was evident during COVID-19 was the stress and need for support for staff and given the restorative or supportive functions of clinical supervision it is a mechanism of support. However, clinical supervisors need support themselves to be able to better meet the supervisee’s needs [ 38 ].
The value of peer group clinical supervision in nurturing a conducive working environment cannot be overstated, as it indorses the understanding and adherence to workplace policies by empowering supervisees to understand the importance and rationale behind these policies [ 39 ]. This becomes vital in a continuously changing healthcare landscape, where guidelines and policies may be subject to change, especially in response to situations such as COVID-19. In an era characterised by international workforce mobility and a shortage of healthcare professionals, a supportive and positive working environment through the provision of peer group clinical supervision can positively influence staff retention [ 40 ], enhance job satisfaction [ 41 ], and mitigate burnout [ 42 ]. A critical aspect of the peer group clinical supervision process concerns providing staff the opportunity to reflect, step back, problem-solve and generate solutions. This, in turn, ensures critical thinking and evaluation within clinical supervision, focusing on understanding the issues and context, and problem-solving to draw constructive lessons for the future [ 30 ]. Research has determined a link between clinical supervision and improvements in the quality and standards of care [ 31 ]. Therefore, peer group clinical supervision plays a critical role in enhancing patient safety by nurturing improved communication among staff, facilitating reflection, promoting greater self-awareness, promoting the exchange of ideas, problem-solving, and facilitating collective learning from shared experiences.
Starting a group arose as a foundational aspect emphasised in this study. The creation of the environment through establishing ground rules, building relationships, fostering trust, displaying respect, and upholding confidentiality was evident. Vital to this process is the recruitment of clinical supervisees and deciding the suitable group size, with a specific emphasis on addressing individuals’ inclination to engage, their knowledge and understanding of peer group clinical supervision, and dissipating any lack of awareness or misconceptions regarding peer group supervision. Furthermore, the educational training of peer group clinical supervisors and the support from external clinical supervisors played a vital role in the rollout and formation of peer group clinical supervision. The evidence stresses the significance of an open and safe environment, wherein supervisees feel secure and trust their supervisor. In such an environment, they can effectively reflect on practice and related issues [ 41 ]. This study emphasises that the effectiveness of peer group supervision is more influenced by the process than the content. Clinical supervisors utilised the process to structure their sessions, fostering energy and interest to support their peers and cultivate new insights. For peer group clinical supervision to be effective, regularity is essential. Meetings should be scheduled in advance, allocate protected time, and take place in a private space [ 35 ]. While it is widely acknowledged that clinical supervisors need to be experts in their professional field to be credible, this study highlights that the crucial aspects of supervision lie in the quality of the relationship with the supervisor. The clinical supervisor should be supportive, caring, open, collaborative, sensitive, flexible, helpful, non-judgmental, and focused on tacit knowledge, experiential learning, and providing real-time feedback.
Critical to the success of peer group clinical supervision is the endorsement and support from management, considering the organisational culture and attitudes towards the practice of clinical supervision as an essential factor [ 43 ]. This support and buy-in are necessary at both the management and individual levels [ 28 ]. The primary obstacles to effective supervision often revolve around a lack of time and heavy workloads [ 44 ]. Clinical supervisors frequently struggle to find time amidst busy environments, impacting the flexibility and quality of the sessions [ 45 ]. Time constraints also limit the opportunity for reflection within clinical supervision sessions, leaving supervisees feeling compelled to resolve issues on their own without adequate support [ 45 ]. Nevertheless, time-related challenges are not unexpected, prompting a crucial question about the value placed on clinical supervision and its integration into the culture and fabric of the organisation or profession to make it a customary practice. Learning from experiences like those during the COVID-19 pandemic has introduced alternative ways of working, and the use of technology (such as Zoom, Microsoft Teams, Skype) may serve as a means to address time, resource, and travel issues associated with clinical supervision.
Despite clinical supervision having a long international history, persistent misconceptions require attention. Some of these include not considering clinical supervision a priority [ 46 ], perceiving it as a luxury [ 41 ], deeming it self-indulgent [ 47 ], or viewing it as mere casual conversation during work hours [ 48 ]. A significant challenge lies in the lack of a shared understanding regarding the role and purpose of clinical supervision, with past perceptions associating it with surveillance and being monitored [ 48 ]. These negative connotations often result in a lack of engagement [ 41 ]. Without encouragement and recognition of the importance of clinical supervision from management or the organisation, it is unlikely to become embedded in the organisational culture, impeding its normalisation [ 39 ].
In this study, some peer group clinical supervisors expressed feelings of being impostors and believed they lacked the knowledge, skills, and training to effectively fulfil their roles. While a deficiency in skills and competence are possible obstacles to providing effective clinical supervision [ 49 ], the peer group clinical supervisors in this study did not report such issues. Instead, their concerns were more about questioning their ability to function in the role of a peer group clinical supervisor, especially after a brief training program. The literature acknowledges a lack of training where clinical supervisors may feel unprepared and ill-equipped for their role [ 41 ]. To address these challenges, clinical supervisors need to be well-versed in professional guidelines and ethical standards, have clear roles, and understand the scope of practice and responsibilities associated with being a clinical supervisor [ 41 ].
The support provided by external clinical supervisors and the peer group clinical supervision sessions played a pivotal role in helping peer group clinical supervisors ease into their roles, gain experiential learning, and enhance their facilitation skills within a supportive structure. Educating clinical supervisors is an investment, but it should not be a one-time occurrence. Ongoing external clinical supervision for clinical supervisors [ 50 ] and continuous professional development [ 51 ] are crucial, as they contribute to the likelihood of clinical supervisors remaining in their roles. However, it is important to interpret the results of this study with caution due to the small sample size in the survey. Generalising the study results should be approached with care, particularly as the study was limited to two regions in Ireland. However, the addition of qualitative data in this mixed-methods study may have helped offset this limitation.
This study highlights the numerous advantages of peer group clinical supervision at individual, service, organisational, and patient/client levels. Success hinges on addressing the initial lack of awareness and misconceptions about peer group clinical supervision by creating the right environment and establishing ground rules. To unlock the full potential of peer group clinical supervision, it is imperative to secure management and organisational support for staff release. More crucially, there is a need for valuing and integrating peer group clinical supervision into nursing and midwifery education and practice. Making peer group clinical supervision accessible to all grades of nurses and midwives across various healthcare services is essential, necessitating strategic planning to tackle capacity and sustainability challenges.
Data availability
Data are available from the corresponding author upon request owing to privacy or ethical restrictions.
Zelenikova R, Gurkova E, Friganovic A, Uchmanowicz I, Jarosova D, Ziakova K, Plevova I, Papastavrou E. Unfinished nursing care in four central European countries. J Nurs Manage. 2020;28(8):1888–900. https://doi.org/10.1111/jonm.12896 .
Article Google Scholar
Department of Health, Office of the Chief Nursing Officer. Position paper 1: values for nurses and midwives in Ireland. Dublin: The Stationery Office; 2016.
Google Scholar
Cummings J, Bennett V. Developing the culture of compassionate care: creating a new vision for nurses, midwives and care-givers. London: Department of Health; 2012.
Both-Nwabuwe JM, Dijkstra MT, Klink A, Beersma B. Maldistribution or scarcity of nurses: the devil is in the detail. J Nurs Manage. 2018;26(2):86–93. https://doi.org/10.1111/jonm.12531 .
Squires A, Jylha V, Jun J, Ensio A, Kinnunen J. A scoping review of nursing workforce planning and forecasting research. J Nurs Manage. 2017;25:587–96. https://doi.org/10.1111/jonm.12510 .
Sasso L, Bagnasco A, Catania G, Zanini M, Aleo G, Watson R. Push and pull factors of nurses’ intention to leave. J Nurs Manage. 2019;27:946–54. https://doi.org/10.1111/jonm.12745 .
Gea-Caballero V, Castro-Sánchez E, Díaz‐Herrera MA, Sarabia‐Cobo C, Juárez‐Vela R, Zabaleta‐Del Olmo E. Motivations, beliefs, and expectations of Spanish nurses planning migration for economic reasons: a cross‐sectional, web‐based survey. J Nurs Scholarsh. 2019;51(2):178–86. https://doi.org/10.1111/jnu.12455 .
Article PubMed Google Scholar
Cutcliffe J, Sloan G, Bashaw M. A systematic review of clinical supervision evaluation studies in nursing. Int J Ment Health Nurs. 2018;27:1344–63. https://doi.org/10.1111/inm.12443 .
Snowdon DA, Hau R, Leggat SG, Taylor NF. Does clinical supervision of health professionals improve patient safety? A systematic review and meta-analysis. Int J Qual Health C. 2016;28(4):447–55. https://doi.org/10.1093/intqhc/mzw059 .
Turner J, Hill A. Implementing clinical supervision (part 1): a review of the literature. Ment Health Nurs. 2011;31(3):8–12.
Dilworth S, Higgins I, Parker V, Kelly B, Turner J. Finding a way forward: a literature review on the current debates around clinical supervision. Contemp Nurse. 2013;45(1):22–32. https://doi.org/10.5172/conu.2013.45.1.22 .
Buss N, Gonge H. Empirical studies of clinical supervision in psychiatric nursing: a systematic literature review and methodological critique. Int J Ment Health Nurs. 2009;18(4):250–64. https://doi.org/10.1111/j.1447-0349.2009.00612.x .
Pollock A, Campbell P, Deery R, Fleming M, Rankin J, Sloan G, Cheyne H. A systematic review of evidence relating to clinical supervision for nurses, midwives and allied health professionals. J Adv Nurs. 2017;73(8):1825–37. https://doi.org/10.1111/jan.13253 .
Snowdon DA, Leggat SG, Taylor NF. Does clinical supervision of healthcare professionals improve effectiveness of care and patient experience: a systematic review. BMC Health Serv Res. 2017;17(1):1–11. https://doi.org/10.1186/s12913-017-2739-5 .
Kühne F, Maas J, Wiesenthal S, Weck F. Empirical research in clinical supervision: a systematic review and suggestions for future studies. BMC Psychol. 2019;7(1):1–11. https://doi.org/10.1186/s40359-019-0327-7 .
Snowdon DA, Sargent M, Williams CM, Maloney S, Caspers K, Taylor NF. Effective clinical supervision of allied health professionals: a mixed methods study. BMC Health Serv Res. 2020;20(1):1–11. https://doi.org/10.1186/s12913-019-4873-8 .
Borders LD. Dyadic, triadic, and group models of peer supervision/consultation: what are their components, and is there evidence of their effectiveness? Clin Psychol. 2012;16(2):59–71.
Health Service Executive. Guidance document on peer group clinical supervision. Mayo: Nursing and Midwifery Planning and Development Unit Health Service Executive West Mid West; 2023.
Sharma A, Minh Duc NT, Lam Thang L, Nam T, Ng NH, Abbas SJ, Huy KS, Marušić NT, Paul A, Kwok CL. Karamouzian, M. A consensus-based checklist for reporting of survey studies (CROSS). J Gen Intern Med. 2021;36(10):3179–87. https://doi.org/10.1007/s11606-021-06737-1 .
Article PubMed PubMed Central Google Scholar
O’Brien BC, Harris IB, Beckman TJ, Reed DA, Cook DA. Standards for reporting qualitative research: a synthesis of recommendations. Acad Med. 2014;899:1245–51. https://doi.org/10.1097/ACM.0000000000000388 .
Winstanley J, White E. The MCSS-26©: revision of the Manchester Clinical Supervision Scale© using the Rasch Measurement Model. J Nurs Meas. 2011;193(2011):160–78. https://doi.org/10.1891/1061-3749.19.3.160 .
Colorafi KJ, Evans B. Qualitative descriptive methods in health science research. HERD-Health Env Res. 2016;9:16–25. https://doi.org/10.1177/1937586715614171 .
Agnew T, Vaught CC, Getz HG, Fortune J. Peer group clinical supervision program fosters confidence and professionalism. Prof Sch Couns. 2000;4(1):6–12.
Mc Carthy V, Goodwin J, Saab MM, Kilty C, Meehan E, Connaire S, O’Donovan A. Nurses and midwives’ experiences with peer-group clinical supervision intervention: a pilot study. J Nurs Manage. 2021;29:2523–33. https://doi.org/10.1111/jonm.13404 .
Rothwell C, Kehoe A, Farook SF, Illing J. Enablers and barriers to effective clinical supervision in the workplace: a rapid evidence review. BMJ Open. 2021;119:e052929. https://doi.org/10.1136/bmjopen-2021-052929 .
Francis A, Bulman C. In what ways might group clinical supervision affect the development of resilience in hospice nurses. Int J Palliat Nurs. 2019;25:387–96. https://doi.org/10.12968/ijpn.2019.25.8.387 .
Chircop Coleiro A, Creaner M, Timulak L. The good, the bad, and the less than ideal in clinical supervision: a qualitative meta-analysis of supervisee experiences. Couns Psychol Quart. 2023;36(2):189–210. https://doi.org/10.1080/09515070.2021.2023098 .
Stacey G, Cook G, Aubeeluck A, Stranks B, Long L, Krepa M, Lucre K. The implementation of resilience based clinical supervision to support transition to practice in newly qualified healthcare professionals. Nurs Educ Today. 2020;94:104564. https://doi.org/10.1016/j.nedt.2020.104564 .
Feerick A, Doyle L, Keogh B. Forensic mental health nurses’ perceptions of clinical supervision: a qualitative descriptive study. Issues Ment Health Nurs. 2021;42:682–9. https://doi.org/10.1080/01612840.2020.1843095 .
Corey G, Haynes RH, Moulton P, Muratori M. Clinical supervision in the helping professions: a practical guide. Alexandria, VA: American Counseling Association; 2021.
Sturman N, Parker M, Jorm C. Clinical supervision in general practice training: the interweaving of supervisor, trainee and patient entrustment with clinical oversight, patient safety and trainee learning. Adv Health Sci Educ. 2021;26:297–311. https://doi.org/10.1007/s10459-020-09986-7 .
Alfonsson S, Parling T, Spännargård Å, Andersson G, Lundgren T. The effects of clinical supervision on supervisees and patients in cognitive behavioral therapy: a systematic review. Cogn Behav Therapy. 2018;47(3):206–28. https://doi.org/10.1080/16506073.2017.1369559 .
Coelho M, Esteves I, Mota M, Pestana-Santos M, Santos MR, Pires R. Clinical supervision of the nurse in the community to promote quality of care provided by the caregiver: scoping review protocol. Millenium J Educ Technol Health. 2022;2:83–9. https://doi.org/10.29352/mill0218.26656 .
Toros K, Falch-Eriksen A. Structured peer group supervision: systematic case reflection for constructing new perspectives and solutions. Int Soc Work. 2022;65:1160–5. https://doi.org/10.1177/0020872820969774 .
Bifarin O, Stonehouse D. Clinical supervision: an important part of every nurse’s practice. Brit J Nurs. 2017;26(6):331–5. https://doi.org/10.12968/bjon.2017.26.6.331 .
Turner J, Simbani N, Doody O, Wagstaff C, McCarthy-Grunwald S. Clinical supervision in difficult times and at all times. Ment Health Nurs. 2022;42(1):10–3.
Martin P, Tian E, Kumar S, Lizarondo L. A rapid review of the impact of COVID-19 on clinical supervision practices of healthcare workers and students in healthcare settings. J Adv Nurs. 2022;78:3531–9. https://doi.org/10.1111/jan.15360 .
van Dam M, van Hamersvelt H, Schoonhoven L, Hoff RG, Cate OT, Marije P. Hennus. Clinical supervision under pressure: a qualitative study amongst health care professionals working on the ICU during COVID-19. Med Edu Online. 2023;28:1. https://doi.org/10.1080/10872981.2023.2231614 .
Martin P, Lizarondo L, Kumar S, Snowdon D. Impact of clinical supervision on healthcare organisational outcomes: a mixed methods systematic review. PLoS ONE. 2021;1611:e0260156. https://doi.org/10.1371/journal.pone.0260156 .
Article CAS Google Scholar
Hussein R, Salamonson Y, Hu W, Everett B. Clinical supervision and ward orientation predict new graduate nurses’ intention to work in critical care: findings from a prospective observational study. Aust Crit Care. 2019;325:397–402. https://doi.org/10.1016/j.aucc.2018.09.003 .
Love B, Sidebotham M, Fenwick J, Harvey S, Fairbrother G. Unscrambling what’s in your head: a mixed method evaluation of clinical supervision for midwives. Women Birth. 2017;30:271–81. https://doi.org/10.1016/j.wombi.2016.11.002 .
Berry S, Robertson N. Burnout within forensic psychiatric nursing: its relationship with ward environment and effective clinical supervision? J Psychiatr Ment Health Nurs. 2019;26:7–8. https://doi.org/10.1111/jpm.12538 .
Markey K, Murphy L, O’Donnell C, Turner J, Doody O. Clinical supervision: a panacea for missed care. J Nurs Manage. 2020;28:2113–7. https://doi.org/10.1111/jonm.13001 .
Brody AA, Edelman L, Siegel EO, Foster V, Bailey DE Jr., Bryant AL, Bond SM. Evaluation of a peer mentoring program for early career gerontological nursing faculty and its potential for application to other fields in nursing and health sciences. Nurs Outlook. 2016;64(4):332–8. https://doi.org/10.1016/j.outlook.2016.03.004 .
Bulman C, Forde-Johnson C, Griffiths A, Hallworth S, Kerry A, Khan S, Mills K, Sharp P. The development of peer reflective supervision amongst nurse educator colleagues: an action research project. Nurs Educ Today. 2016;45:148–55. https://doi.org/10.1016/j.nedt.2016.07.010 .
Pack M. Unsticking the stuckness’: a qualitative study of the clinical supervisory needs of early-career health social workers. Brit J Soc Work. 2015;45:1821–36. https://doi.org/10.1093/bjsw/bcu069 .
Bayliss J. Clinical supervision for palliative care. London: Quay Books; 2006.
Kenny A, Allenby A. Implementing clinical supervision for Australian rural nurses. Nurs Educ Pract. 2013;13(3):165–9. https://doi.org/10.1016/j.nepr.2012.08.009 .
MacLaren J, Stenhouse R, Ritchie D. Mental health nurses’ experiences of managing work-related emotions through supervision. J Adv Nurs. 2016;72:2423–34. https://doi.org/10.1111/jan.12995 .
Wilson HM, Davies JS, Weatherhead S. Trainee therapists’ experiences of supervision during training: a meta-synthesis. Clinl Psychol Psychother. 2016;23:340–51. https://doi.org/10.1002/cpp.1957 .
Noelker LS, Ejaz FK, Menne HL, Bagaka’s JG. Factors affecting frontline workers’ satisfaction with supervision. J Aging Health. 2009;21(1):85–101. https://doi.org/10.1177/0898264308328641 .
Download references
Acknowledgements
The research team would like to thank all participants for their collaboration, the HSE steering group members and Carmel Hoey, NMPDU Director, HSE West Mid West, Dr Patrick Glackin, NMPD Area Director, HSE West, Annette Cuddy, Director, Centre of Nurse and Midwifery Education Mayo/Roscommon; Ms Ruth Hoban, Assistant Director of Nursing and Midwifery (Prescribing), HSE West; Ms Annette Connolly, NMPD Officer, NMPDU HSE West Mid West.
The authors declare that there are no sources of funding associated with this paper.
Author information
Authors and affiliations.
Department of Nursing and Midwifery, Health Research Institute, University of Limerick, Limerick, Ireland
Owen Doody, Kathleen Markey, Claire O. Donnell & Louise Murphy
Department of Nursing and Midwifery, Sheffield Hallam University, Sheffield, UK
James Turner
You can also search for this author in PubMed Google Scholar
Contributions
OD: Conceptualization, Methodology, Formal analysis, Investigation, Writing - Original Draft, Writing - Review & Editing, Project administration, Funding acquisition. COD: Methodology, Formal analysis, Investigation, Writing - Original Draft, Writing - Review & Editing, Funding acquisition. KM: Methodology, Formal analysis, Investigation, Writing - Original Draft, Writing - Review & Editing, Funding acquisition. JT: Methodology, Formal analysis, Writing - Original Draft, Writing - Review & Editing. LM: Methodology, Formal analysis, Investigation, Writing - Original Draft, Writing - Review & Editing, Funding acquisition.
Corresponding author
Correspondence to Owen Doody .
Ethics declarations
Ethics approval and consent to participate.
This study was approved by two health service institutional review boards University Hospital Limerick (Ref: 091/19) and Galway University Hospitals (Ref: C.A. 2199). The study was conducted in accordance with the principles of the Declaration of Helsinki and all study details were fully disclosed to participants, who were assured of the voluntary nature of participation and withdrawal. The study questionnaires were coded, and identities were not disclosed to guarantee participants’ anonymity and all participants provided written informed consent before interviews.
Consent for publication
No identifying images or other personal or clinical details of participants are presented in this paper that would compromise anonymity and all participants were aware and informed through the Participant Information Leaflet that the data collected may be reported through article and/or conference publications and this was reiterated during the qualitative data collection stage.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary material 2, supplementary material 3, rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/ .
Reprints and permissions
About this article
Cite this article.
Doody, O., Markey, K., Turner, J. et al. Clinical supervisor’s experiences of peer group clinical supervision during COVID-19: a mixed methods study. BMC Nurs 23 , 612 (2024). https://doi.org/10.1186/s12912-024-02283-3
Download citation
Received : 04 January 2024
Accepted : 22 August 2024
Published : 02 September 2024
DOI : https://doi.org/10.1186/s12912-024-02283-3
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Clinical supervision
BMC Nursing
ISSN: 1472-6955
- General enquiries: [email protected]
IMAGES
VIDEO
COMMENTS
Types of Interviews in Research | Guide & Examples. Published on March 10, 2022 by Tegan George. Revised on June 22, 2023. An interview is a qualitative research method that relies on asking questions in order to collect data. Interviews involve two or more people, one of whom is the interviewer asking the questions.
Qualitative Sociology 37(2):153-171. Written as a response to various debates surrounding the relative value of interview-based studies and ethnographic studies defending the particular strengths of interviewing. This is a must-read article for anyone seriously engaging in qualitative research! Pugh, Allison J. 2013.
Interviews, in general, are a foundational means of collecting data when using qualitative research methods. They are designed to draw from the interviewee constructs embedded in his or her thinking and rationale for decision making. The researcher uses an inductive method in data gathering, regardless of whether the interview method is open ...
An interview is a qualitative research method that relies on asking questions in order to collect data. Interviews involve two or more people, one of whom is the interviewer asking the questions. There are several types of interviews, often differentiated by their level of structure.
There are different types of interviews that can be used in qualitative research, including structured interviews, semi-structured interviews, and unstructured interviews. Each type of interview has its own advantages and is suitable for different research objectives and contexts.
In-depth interviews are a qualitative research method that follow a deceptively familiar logic of human interaction: ... given that different researchers will elicit different types of data from ...
Abstract. Qualitative interviewing is a foundational method in qualitative research and is widely used in health research and the social sciences. Both qualitative semi-structured and in-depth unstructured interviews use verbal communication, mostly in face-to-face interactions, to collect data about the attitudes, beliefs, and experiences of ...
Interviews are the most common data collection technique in qualitative research. There are four main types of interviews; the one you choose will depend on your research question, aims and objectives. It is important to formulate open-ended interview questions that are understandable and easy for participants to answer.
This short video summarizes why interviews can serve as useful data in qualitative research. InterViews by Steinar Kvale Interviewing is an essential tool in qualitative research and this introduction to interviewing outlines both the theoretical underpinnings and the practical aspects of the process. After examining the role of the interview ...
Interviews are the most commonly used qualitative data gathering technique and are used with grounded theory, focus groups, and case studies. The length of an interview varies. They may be anywhere from thirty minutes to several hours in length, depending on your research approach. Structured interviews use a set list of questions which need to ...
A qualitative research interview is a one-to-one data collection session between a researcher and a participant. Interviews may be carried out face-to-face, over the phone or via video call using a service like Skype or Zoom. There are three main types of qualitative research interview - structured, unstructured or semi-structured.
Interviews, as a qualitative research method, play a pivotal role in uncovering complexities in human behavior and decision-making. Researchers can observe behavior, on the one hand, or they can investigate the perspectives and values informing that behavior by interviewing research participants.
Interviewing. This is the most common format of data collection in qualitative research. According to Oakley, qualitative interview is a type of framework in which the practices and standards be not only recorded, but also achieved, challenged and as well as reinforced.[] As no research interview lacks structure[] most of the qualitative research interviews are either semi-structured, lightly ...
Here are some steps on how to analyze a qualitative interview: 1. Transcription. The first step is transcribing the interview into text format to have a written record of the conversation. This step is essential to ensure that you can refer back to the interview data and identify the important aspects of the interview.
It is the most widely used method in qualitative research. It is flexible, inexpensive, and does not inter-fere with the researcher's life the way that ethnography does. This chapter looks at qualitative interviewing and how it compares to other types of collect-ing evidence in research, particularly structured interviewing and ethnography.
Qualitative research is an approach that focuses on people and their experiences, behaviours and opinions. 10,11 The qualitative researcher seeks to answer questions of 'how' and 'why', providing ...
Three types of interviews: Qualitative research methods in social health Heather L. Stuckey Department of Medicine and Public Health Sciences, Pennsylvania State University College of Medicine, PA 17033, USA ... Key words: Interviews, qualitative research, social health Access this article online Website: www.joshd.net DOI: 10.4103/2321-0656.115294
Semistructured Interviews. These are interviews that use an interview protocol to help guide the researcher through the interview process. While this can incorporate conversational aspects, it is mostly a guided conversation between the researcher and participant. It does maintain some structure (hence the name semistructured), but it also ...
Qualitative research methods. Each of the research approaches involve using one or more data collection methods.These are some of the most common qualitative methods: Observations: recording what you have seen, heard, or encountered in detailed field notes. Interviews: personally asking people questions in one-on-one conversations. Focus groups: asking questions and generating discussion among ...
Qualitative Research. Qualitative research is a type of research methodology that focuses on exploring and understanding people's beliefs, attitudes, behaviors, and experiences through the collection and analysis of non-numerical data. It seeks to answer research questions through the examination of subjective data, such as interviews, focus ...
Three types of interviews are common in social health: (1) Structured; (2) semi‑structured; and (3) narrative interview. These range in a format including speci ed sets of questions to the ...
It's possible the historical data isn't relevant enough to gather useful data from in a post-pandemic world. 6. Narrative model. The narrative method is one of the types of qualitative research methods that focuses on written and spoken words or visual representations by people. Here, stories become raw data.
Qualitative research types provide valuable insights through a variety of methods focused on understanding human behavior, emotions, and experiences. Among the most popular types are interviews, focus groups, ethnography, and case studies. Each method offers unique advantages in collecting data that reflects the subjective perspectives of ...
This paper has explored various types of elicitation strategies in qualitative research and demonstrated that timeline drawing elicitation has proven to be an impactful strategy in phone and ... Tools and typologies for the use of participant-led diagrams in qualitative research interviews. Qualitative Research, 19(5), 506-523. https://doi ...
Data collection at live events has used a wide variety of methods from a range of disciplines in contemporary research, but this was predominantly via quantitative or secondary research approaches (see Draper et al., 2018; Getz, 2010; Park & Park, 2017). Mair (2012) highlighted that qualitative methodologies were significantly underrepresented in high impact journals, and the event research ...
Our interview study formed the first phase of a multi-method qualitative inquiry into the working practices of NIHR-funded PPI leads. While PPI lead posts are in evidence in most NIHR-funded research, we decided to focus on NIHR infrastructure funding specifically: these are 5-year grants absorbing a major tranche of NIHR funds (over £600 million annually in 2024).
Method This was a secondary thematic analysis of 46 qualitative interviews conducted online/by telephone to explore primary care practitioners' experiences of supporting women's health needs in general practice, alongside consultation with representatives of a lived-experience group to contextualise the findings. ... Qualitative research ...
You should choose this type of interview when your study is focused on one research approach and you want to have the same structure of the interview for all participants. The Study Interviews are all about the study which is connected to the interview. When you create a study interview, you need to choose one of the 9 available study types.
This study fills this gap by examining the barriers to GRS across different industries in China. It adopted a qualitative and inductive approach, which is relatively rare in the GHRM field. Based on interviews with senior managers, a number of barriers were revealed in relation to the two components of GRS: paperless recruitment and green ...
Background Providing positive and supportive environments for nurses and midwives working in ever-changing and complex healthcare services is paramount. Clinical supervision is one approach that nurtures and supports professional guidance, ethical practice, and personal development, which impacts positively on staff morale and standards of care delivery. In the context of this study, peer ...